ISSN : 2472-1905
Journal of Aesthetic & Reconstructive Surgery
Flap reconstruction of rectovaginal and rectourethral fistulas: A 20-years experience
2nd International Conference on Plastic & Aesthetic Surgery
July 27-28, 2017 Vancouver, Canada
Jeremie D Oliver, Arya A Akhavan, Z S Hammoudeh, Eric D Hokenstad, Nho V Tran and J A Occhino
Mayo Clinic, USA UNC Medical Center, USA
Posters & Accepted Abstracts: J Aesthet Reconstr Surg
Abstract
Background: Rectovaginal and rectourethral fistulas can occur secondary to obstetric complications, cancer and radiation, inflammatory bowel disease, and previous surgery. They are highly distressing to the patient and are often refractory to treatment. Flap reconstruction places vascularized tissue between the apertures, creating separation and aiding in healing. This is particularly useful for complex cases refractory to standard techniques.
Aim: The purpose of this study was to investigate the outcomes of flap reconstruction of rectovaginal and rectourethral fistulas in the setting of complicating comorbidities.
Methods: All patients at all Mayo Clinic hospitals who underwent flap reconstruction of a rectovaginal or rectourethral fistula between January 1995 and December 2014 were identified. Patient demographics, surgical indications, and comorbidities were collected. Operative and postoperative data were also collected, including flap type, length of hospital stay, 30-day complications, recurrences, and follow-up time. Operative success was defined as definitive treatment of the fistula without recurrence within 6 months.
Results: There were 59 patients who underwent 66 reconstructions. The 30-day postoperative complication rate was 59.1% across all patients, primarily consisting of infection (13) and dehiscence (11), with only 1 partial flap loss and no mortality. The 6-month success rate was 51.5% across all patients. Patients with fistula secondary to obstetric complications had significantly lower success rates (11.1%, p=0.031). There were no other statistically significant differences in outcomes by etiology, history of radiation, flap type, gender, or history of prior repair attempt.
Conclusions: Flap reconstruction remains a valuable treatment option for complex or refractory rectovaginal, rectourethral, and other GI-to-genitourinary or complex genitourinary-perineal fistulas. Many different flaps, including low-morbidity options such as gracilis and Martius-type flaps, can successfully be used as first-line reconstructive options. Despite an initial success rate of 50%, nearly all cases were able to be repaired after a single additional reconstructive procedure. Patients with GI-to-vaginal fistulas due to obstetric complications had significantly lower success rates.
Biography
E-mail: oliver.jeremie@mayo.edu
Google Scholar citation report
Citations : 130
Journal of Aesthetic & Reconstructive Surgery received 130 citations as per Google Scholar report
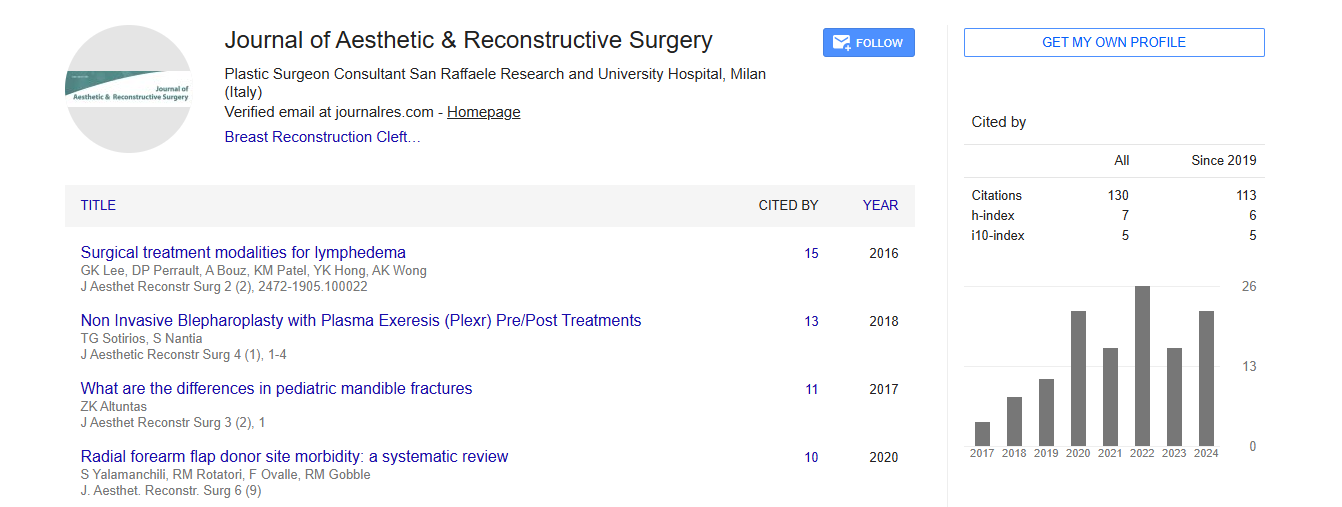
Journal of Aesthetic & Reconstructive Surgery peer review process verified at publons
Abstracted/Indexed in
- Google Scholar
- China National Knowledge Infrastructure (CNKI)
- Directory of Research Journal Indexing (DRJI)
- WorldCat
- Publons
- Geneva Foundation for Medical Education and Research
- Secret Search Engine Labs
- Euro Pub
Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences