Closed Loop Control: A Newer Mode of Mechanical Ventilation
Umesh K Bylappa*, Abdul Aziz M Alhashemi, Chokkalinga Damodaran, Thiruppathi Chockalingam and Hussam A Ghali
Respiratory Therapist, Respiratory Therapy Department, Hamas General Hospital, Doha, Qatar
- *Corresponding Author:
- Umesh K Bylappa
Respiratory Therapist
Respiratory Therapy Department
Hamas General Hospital
Doha, 3050, Qatar
Tel: +974-44342292
E-mail: ubylappa@hamad.qa
Received Date: June 28, 2017; Accepted Date: July 20, 2017; Published Date: July 27, 2017
Citation: Bylappa UK, Alhashemi AAM, Damodaran C, Chockalingam T, Ghali HA (2017) Closed Loop Control: A Newer Mode of Mechanical Ventilation. J Clin Med Ther. 2:18.
Abstract
Closed loop control ventilation is a dual control mode of ventilation, which uses a closed loop control technique. This mode delivers controlled, time triggered, time cycled breaths when patient is not breathing and patient triggered flow cycled breaths when a patient is breathing. If the patient has spontaneous breaths, it delivers flow cycled breaths and allows the patient to trigger and breathe spontaneously, either in between the controlled breaths or fully spontaneously. This mode is pressure limited for control, assist control and spontaneous breath. The pressure will be varying and depends on the target tidal volume and uses auto-flow throughout the cycle. INTELLiVENT is a closed loop mode of ventilation, an advance over the closed loop control mode where the ventilator automatically adjusts settings and optimizes ventilation depending on the target settings and physiological information from the patient.
Keywords
Ventilation; Spontaneous breath; INTELLiVENT; Respiratory rate
Introduction
In latest version of positive pressure mechanical ventilation, there are two ways to control the variables. They are closed loop control variable and open loop control variable. The closed loop control mode, which is closed loop control mechanical ventilation, is based on the information on respiratory mechanics of the patient. The resistance and compliance of the lungs are measured continuously breath by breath to control the pressure and deliver a target volume.
In the closed loop control system, the pressure and flow of gases from the ventilator (output) are measured and matched with the pressure and flow of gases back into the ventilator (input), based on which subsequent output is adjusted. The feedback control forces the pressure and flow of gases to become stable in the presence of changes in compliance, resistance of the lung and respiratory muscle fatigue. In this mode of ventilation, the ventilator is also programmed to incorporate lung protection strategies.
Feedback System
The operator inputs details such as the patient’s age, gender and height into the system through which minute ventilation is calculated and sets a Target Volume (VT) and Respiratory Rate (RR) through a feedback signal. The systems gives test breath in which target tidal volume of the patient is observed and stored in the system. The observed tidal volume and target tidal volume are compared according to the lung mechanics and then target tidal volume for the patient is decided depending on lung compliance, resistance and expiratory time constant.
Other closed loop ventilator modes are Neurally Adjusted Ventilatory Assistance (NAVA), Proportional Assist Ventilation (PAV), Knowledge-Based Systems (KBS). These are modifications of pressure support mode and mainly used in spontaneously breathing patients for weaning.
INTELLiVENT is distinctly different in that it can be used for any patient, whether breathing or not. The ventilation proceeds automatically and can be described as three different modes rolled into one [1]. If the patient is not breathing, it acts as pressure control mode. If patient is breathing spontaneously in between the control breaths, but the spontaneous breaths are less than the target respiratory rate, it acts as synchronized intermittent mandatory ventilation and pressure support mode. If patient is breathing well spontaneously and the spontaneous respiratory rates are higher than the target rate, it acts as pressure support mode.
History
Closed loop ventilation was introduced initially in the form of mandatory minute Ventilation (MMV) by Hewlett [2]. Minute ventilation appropriate for the patient had to be chosen by the user. The machine would monitor the patient’s respiratory rate and tidal volume. As long as the patient’s respiratory pattern remained above the MMV line (a diagonal line drawn from time zero to reach the target minute ventilation at the end of one minute on a graph with time on the X-axis and minute ventilation on the Y-axis), the ventilator would remain passive. If at any time, the patient respiration was observed to drop below the line, the ventilator would deliver extra breaths at the preset tidal volume to ensure that the respiration returned to remain above the line. The augmentation of tidal volume could be achieved by using pressure support also. Mandatory minute ventilation was designed to be a weaning mode and was meant to encourage the patient’s spontaneous ventilation. One of the draw backs of this ventilation was that the patient could cheat the ventilator with rapid and shallow breaths [3].
Closed loop control ventilation was originally described by Tehrani (clinical engineering Professor at the University of California, USA) [4]. This was the first commercially available ventilator that used an ‘optimal’ targeting scheme [5]. A modified version of Otis equation is used to determine the optimum frequency of mechanical ventilation to minimize the work of breathing [6]. The rationale was to make the patient's breathing pattern comfortable and natural within safe limits, stimulate spontaneous breathing and reduce the weaning time. Thus closed loop control ventilation replaces open loop control ventilatory modes.
Closed Loop Control Concept
Closed loop control uses closed loop mechanism to switch between spontaneous and controlled breaths. In this mode of ventilation, the ventilator adapts itself to the patient by continuous assessment and provides support as required by the patient to minimize work of breathing. Closed loop control can be used to provide full or partial ventilator support during initiation, maintenance or weaning from mechanical ventilation.
Mechanism of Closed Loop Control
The user has to feed in details such as the patient’s age group, whether an adult, child or an infant, gender and height. The patient’s ideal body weight is then calculated and displayed by the ventilator. The clinician must then set the target minute ventilation (20-200%), in terms of percentage of the normal minute ventilation based on the patient’s ideal body weight and the maximum plateau pressure, also called the closed loop control pressure limit. Positive end-expiratory pressure and the inspired Fraction of oxygen (FIO2) must also be set. The maximum pressure alarm (Pmax) must be set 10 cm H2O above the closed loop control pressure alarm limit.
Based on the patient’s lung compliance, airway resistance, and dead space as calculated using the Radford nomogram, an optimal minute ventilation, tidal volume and frequency that would minimize the work of breathing is calculated by the ventilator using Otis equation. It constructs a safety ventilation window within which the patient is allowed to breathe. If a patient’s respiratory pattern falls outside of this window, the ventilator provides assistance in the form of number of mandatory breaths or by providing pressure support to each breath as necessary. Since both the volume and pressure targets are defined, the use of closed loop control reduces volutrauma and barotrauma.
Otis Equation
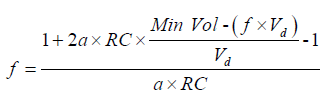
f=Respiratory rate; RC=Airway resistance × Respiratory compliance=Time constant; Min Vol=Minute ventilation; Vd=dead space; a=(2π2)/60=0.33.
Otis equation is used to calculate respiratory rate as seen in Figure 1. Point A represents very low respiratory rate with high tidal volume to maintain the adequate targeted alveolar minute ventilation. Point B represents maintenance of adequate targeted alveolar minute ventilation at very high respiratory rate and low tidal volume. Point C represents very minimal work of breathing to maintain adequate targeted alveolar minute ventilation with normal tidal volume and respiratory rate.

Figure 1: Respiratory rate, tidal volume and work of breathing.
Tidal Volume against Respiration Rate
As described above, closed loop control mode uses Otis equation to calculate target respiratory rate and tidal volume. Closed loop control mode selects respiratory rate and tidal volume depending on the lung mechanics. It selects low respiratory rate, high tidal volume in case of obstructive lung diseases and low tidal volume, high respiratory rate in case of restrictive lung diseases [2].
One of the main parameters which determine the respiratory rate and tidal volume is expiratory time constant, a product of airway resistance and compliance. It is calculated continuously by the analysis of flow-volume curve, based on which the I:E ratio, target rate and target volume are set and a safety window is created using mathematical calculations [7]. One expiratory time constant indicates the time taken for movement of 63% of the volume to move out of the lungs and three time constants are required to move 95% of the volume out of the lungs.
Closed Loop Control Ventilation- Operating Principles
Closed loop control mode follows, implements and works on the basis of lung protective strategies, which targets respiratory rate and tidal volume within the safety margin of window. This way it can avoid and prevent complications like volutrauma, barotrauma, intrinsic PEEP (Positive end expiratory pressure) and/or dead space ventilation (Figure 2).

Figure 2: Lung protective strategies.
The following safety limits are calculated automatically based on the operating principles (Table 1).
| Safety Limits | ||
|---|---|---|
| Setting | Minimum | Maximum |
| Inspiratory Pressure | 5 cm Above PIP | 10 cm Under P. max |
| Tidal Volume | 4.4 × IBM | 15.4 IBM Limited P. max |
| RR Target | 5 RR/min | 60 RR/min |
| Inspiratory Time | 0.5 s | 2 s |
| Expiratory Time | 3 s | 12 s |
| I:E Ratio | 01:04 | 01:01 |
Table 1: Safety limits.
Closed Loop Control Ventilation- General Principles
The closed loop control ventilation mode adapts and changes according to patient’s respiratory effort. If the patient is not breathing or triggering even a single breath, it delivers mandatory breaths and works as pressure control mode (PCV-time triggered, pressure limited and time cycled ventilation). If the ventilator senses or measures spontaneous respiratory rate, which is less than target respiratory rate, then it works as pressure control synchronized intermittent mandatory ventilation (SIMV) plus pressure support mode (P-SIMV+PS). If the patient’s spontaneous respiratory rate is more than the target respiratory rate, it is assumed that the work of breathing is high and each breath is supported using pressure support mode (PS-patient triggered, pressure limited and flow cycled ventilation).
Closed loop control Mode continuously measures respiratory mechanics and maintains ventilator parameters within the safety limits. During the Pressure Support (PS) ventilation in the closed loop ventilation, if the patient is not breathing or the spontaneous respiratory rate is less than the target respiratory rate, it automatically increases the pressure controlled mandatory breaths which is required to maintain the target minute ventilation. With the interaction of closed loop control mode, it also limits or controls too high or too low respiratory rate and tidal volume to prevent or minimize hypoventilation or hyperventilation, dead space volume, barotrauma and auto PEEP (Positive end expiratory pressure).
Closed Loop Control Settings
The initial ventilator settings of closed loop control are given in Table 2.
| Height of the Patient | In Centimetre |
|---|---|
| Gender | Male or Female |
| Minute Volume in Percentage | 25-350% |
| Normal | 100% |
| Restrictive Lung Disease | 120% |
| Obstructive Lung Disease | 90% |
| Trigger | 2 to 5 l/min |
| Expiratory Trigger Sensitivity | 25% to 40% |
| Tube Resistance Compensation | Set to 100% |
| High Pressure Alarm Limit | Above 10 cm water |
| PEEP & FiO2 | As Per Clinical Condition |
Table 2: Closed loop control ventilator settings.
At the start of closed loop control mode of ventilation, the ventilator gives a minimum of three test breaths with the PC of more than 15 cm H2O. During these test breaths, it measures inspiratory time (Ti), inspiratory pressure (Pinsp), compliance and resistance of the respiratory system to calculate expiratory time constant and uses these parameters with the estimated dead space volume and minute ventilation which are calculated on the basis of ideal body weight and calculates target respiratory rate. Finally with these measurements, it sets target tidal volume and respiratory rate within the safety window [8]. During ventilation, depending on the lung mechanics the pressure limit increases or decreases within the set closed loop control pressure limit to achieve target tidal volume. Oxygenation and ventilation (MV%) can be adjusted manually according to the clinical parameters.
Optimization and Controlling Of MV% (Minute Ventilation)
Optimization and controlling of MV depends on the patient’s effort and the arterial blood gases results. Percentage of minute ventilation can be altered depending on the arterial carbon dioxide level and the total minute ventilation the patient generates including minute ventilation delivered by the ventilator. MV% can be weaned depending on the patient effort and spontaneous breaths. As discussed earlier, if the patient’s RR is more than the target RR, it means patient is breathing on PS level. The PS level and patient effort can be seen on the ventilator monitor to decide on weaning [3-11]. Even with the closed loop ventilation there are advantages and disadvantages mentioned in Table 3.
| Advantages | Disadvantages |
|---|---|
| Can ventilate any group | Inability to recognize and adjust Δ in Alveolar dead space ventilation |
| Guaranteed TV and MV | Variable peak pressure |
| Safe-prevents tachycardia, Audio-PEEP, Dead space | In patients with COPD, a longer TE may be required |
| Less operator dependent | Cannot directly program VT, RR, I:E ratio |
| Decrease time on mechanical ventilation | Limited pediatric experience |
| Minimal patient WOB | Algorithm tends to ventilate with TV and high RR |
| Weaning is done automatically and continuously | Only available with Hamilton ventilator |
| Variable flow to meet patient demand | |
| Decelerating flow waveform to improve gas distribution | |
Table 3: Advantages and disadvantages.
INTELLiVENT-Closed Loop Control Ventilation
INTELLiVENT-closed loop control is a fully automatic ventilation mode [12]. It is closed loop control mode which uses some additional special settings to autopilot the ventilation.
In this mode, oxygenation and ventilation settings are set automatically (MV, PEEP, FiO2) according to target end-tidal carbon dioxide levels (EtCO2) and oxygen saturation (SpO2). Thus the ventilator adjusts the settings according to the patient’s clinical condition which can change dynamically such as general conditions, underlying diseases, ventilatory demand, respiratory mechanics and spontaneously breathing activities.
INTELLiVENT-closed loop control has five interrelated functions which are auto adjustment for CO2 elimination, auto adjustment for oxygenation, auto weaning tool including quick wean, SBT trial and heart lung index. The setting of target minute volume is automated based on either the monitored EtCO2 or the monitored spontaneous breathing rate. The auto adjustment of FiO2 or PEEP is based on the monitored SpO2 with pulse oximeter, pulse oximetry using a finger or ear probe. The goal is to keep EtCO2, spontaneous rate and SpO2 within the predicted target ranges. The combination of PEEP and FiO2 is selected according to a table derived from ARDS network publications. Tidal volume and respiratory rate are determined by the time-proven closed loop control ventilation algorithm, based on the least work of breathing.
INTELLiVENT-closed loop control ensures that the patient is never apnoeic, does not get too large or too low tidal volumes, too high or too low respiratory rate and also ensures that the airway pressures are maintained within limits, thus complying with lung protective strategies, avoid volutrauma, barotrauma, auto-PEEP, dead space ventilation and also aid in quicker weaning.
Weaning with INTELLiVENT-Closed Loop Control Ventilation
INTELLiVENT-closed loop control provides an optional automated weaning protocol, called Quick Wean. Quick Wean progressively reduces pressure support, monitors for the readiness-to-wean criteria, and provides an operator configurable weaning protocol. Quick Wean also includes the option to automatically conduct fully controlled Spontaneous Breathing Trials (SBT).
Heart Lung Index (HLI)
HLI is a new and special parameter of INTELLiVENT-closed loop control to indicate the extent to which the haemodynamics are affected by the applied positive pressure. HLI is based on automatic analysis of variations in the monitored pulse oximeter plethysmogram and is expressed in percentage (Figure 3) [12]. If HLI is more than 15%, the currently delivered mechanical ventilation may have a strong influence on the haemodynamics. Currently, the HLI is available only when a Nihon Kohden SpO2 sensor is in use.

Figure 3: Pulse pressure variation.
Unique Spo2 Option Featuring Advanced Artefact Rejection and Heart- Lung Interaction Index
The INTELLiVENT uses the principle of pulse pressure variation (PPV) for the assessment of haemodynamic status. The pulse oximeter compatible with the ventilator (Hamilton Medical) is from Nihon Kohden. It incorporates advanced automatic rejection of artefacts that may be seen with the use of pulse oximeter to increase accuracy of the measurement of PPV. It thus increases safety of the closed loop ventilation using this parameter with the added advantage of continuous noninvasive monitoring of the haemodynamic status. The interaction between the respiratory and cardiovascular systems is displayed as heart lung index (HLI).
Closed Loop Control Ventilation as Weaning and Lung Protective Strategy
Several studies have evaluated adaptive support ventilation for weaning.
Morato et al. conducted a study comparing adaptive support ventilation, mandatory rate ventilation and Smartcare for automated weaning from mechanical ventilation [13]. They evaluated these three modes in six different weaning situations: weaning success, weaning failure, weaning success along with extreme anxiety, weaning success along with Cheyne-Stokes breathing, weaning success along with irregular breathing and weaning failure along with ineffective efforts. All three modes performed equally well in all the situations but the adjustment of pressure support from ASV was faster (1-2 min) and was slowest with Smartcare (8-78 min).
Zhu et al. adaptive support ventilation mode with physician directed weaning in patients after fast-track cardiac valvular surgery [14]. Adjustment of ASV (Adaptive support ventilation) were made based on arterial blood gas analysis whereas all decisions were made by physicians in the physician directed weaning. They found that the use of ASV (Adaptive support ventilation) shortened weaning time by at least 2 h and reduced number of alarms and manual ventilator changes.
Mohamed and Maraghi compared the role of adaptive support ventilation and pressure support ventilation in weaning of COPD (Chronic obstructive pulmonary disease) patients [15]. Once the patients had recovered with medical therapy and assist control mode of ventilation, they were randomized to be weaned off ventilation with either ASV of PSV (Pressure support ventilation). They found that weaning with ASV was faster, and length of stay in ICU as well as in the hospital was significantly reduced.
Arna et al. evaluated the use of INTELLiVENT-ASV as a fully closed loop ventilation mode in 100 unselected patients in the ICU requiring at least 12 h of mechanical ventilation [16]. All adjustments were made by the ventilator and they found the ventilator setting changes were different for different conditions and were all appropriate in all patients including normal lungs, COPD (Chronic obstructive pulmonary disease) and ARDS (Acute respiratory distress syndrome). They concluded that the use of IntelliVent-ASV was safe in all these conditions.
Elmorsy et al. compared adaptive support ventilation with biphasic positive airway pressure for ventilating patients with acute exacerbation of chronic obstructive pulmonary disease [17]. There were 36 patients in each group. They found that in the ASV group, the respiratory rate was significantly lower, tidal volume was higher, and rapid shallow breathing index was lower. Lung compliance was higher, airway resistance lower and patient-ventilator synchrony was better with ASV. Days of mechanical ventilation and duration of ICU stay was found to be less with ASV.
Chen et al. conducted a study to compare effects of implementing adaptive support ventilation in a medical intensive care Unit [18]. They compared 79 patients who underwent weaning using AVS with 70 patients being weaned off using conventional ventilation. They found that weaning readiness was not recognized in 15% of patients when ventilated with conventional modes. They also opined that ASV helps to identify these patients and may improve their weaning outcomes.
Cabodevila et al. conducted a study evaluating selection of ventilator settings by humans versus computers in adaptive support ventilation and Mid-frequency Ventilation (MFV) in different clinical scenarios [19]. Although there were differences in the initial ventilator settings where the tidal volumes selected by the physicians were slightly lower, the inspiratory pressures were lower with ASV and MFV. Overall, the three sets of selection of parameters were similar.
Sulemanji et al. compared adaptive support ventilation where the plateau pressure was limited to 28 cm H2O and conventional volume controlled ventilation with a fixed tidal volume of 6 ml/kg in a lung simulator model [10]. The different scenarios examined were a positive end-expiratory pressure of 8, 12 and 16 cm H2O and in two groups: Group 1 for 60 kg and Group 2 for 80 kg. ASV was better able to maintain plateau pressure by changing tidal volumes and could be considered as a safe mode of ventilation in these patients.
Gruber et al. conducted a randomized controlled trial comparing ASV with pressure regulated volume control in the auto mode in 50 patients who had undergone uncomplicated cardiac surgery [20]. They looked at the days of intubation, mechanical ventilation and number of physician interventions during weaning. They found that the use of ASV resulted in earlier extubation, without an increase in clinician intervention.
Other Benefits of Closed Loop Control Ventilation
Sviri et al. in their paper in 2012 describe how they have used ASV as a mode of ventilation in their ICU and also that it had become the primary or preferred mode of ventilation for all their patients for the last ten years [21]. They had the experience of ventilating more than 1000 patients with ASV. 81% could be successfully weaned, 6% had to be switched over to pressure controlled ventilation because they were hypoxic, needed high inspiratory pressures and had to be administered nitric oxide. Only <1% ventilated with ASV developed pneumothorax whereas the overall incidence of pneumothorax was 3%. They opined that ASV is a safe and acceptable mode of ventilation for complicated medical patients, with a lower than usual ventilation complication rate.
Agarwal et al. did a randomized controlled trial comparing ASV with volume controlled ventilation in 48 patients with acute respiratory distress syndrome [22]. They found both modes to be similar in all aspects of mechanical ventilation such as duration of mechanical ventilation, organ dysfunction and mortality.
Summary
Closed loop control ventilation is a dual control mode of ventilation. As the name implies, it automatically changes the mode from control to spontaneous, spontaneous to control, depending on the patient’s effort. It prevents tachypnoea, low tidal volume high respiratory rate ventilation, intrinsic PEEP and excessive dead space ventilation. So it can be used in any patient, from the initiation to cessation of ventilation without changing modes. It also delivers the target tidal volume while increasing or decreasing pressure control or pressure support level without exceeding the plateau pressure which is closed loop control pressure limit set by the clinician.
Closed loop control uses lung protective strategy to minimize the lung injury. It can be used in both obstructive and restrictive lung disease patients for initiation, maintenance and weaning from mechanical ventilation. However, presently there are not many researches to support closed loop control ventilation in severely ill chronic patients to show any mortality benefit.
Several studies conducted on INTELLiVENT-closed control loop ventilation is an automated mode which controls oxygenation and ventilation itself while increasing and decreasing minute ventilation, PEEP and FiO2. It keeps the lungs under protective ventilation strategy and also results in earlier extubation, without an increase in clinician intervention. Also reduces days of mechanical ventilation and duration of ICU stay of the patient.
Conclusion
INTELLiVENT closed-loop control automation is based on the closed-loop control principle with monitored PetCO2, spontaneous rate and SpO2 inputs. Use of INTELLiVENT closed-loop control can improve the quality of mechanical ventilation and unburden the clinical staff from frequent manipulation of the ventilator controls. However randomized control studies are required to prove the effect on mortality apart from the obvious short term benefit it offers. Also closed loop ventilation can be used from intubation to extubation while using manual settings of MV, FiO2 and PEEP without changing mode.
References
- Wysocki M, Brunner JX (2007) Closed-loop ventilation: An emerging standard of care? Crit Care Clin 23: 223-240.
- Hewlett AM, Platt AS, Terry VG (1977) Mandatory minute volume. A new concept in weaning from mechanical ventilation. Anaesthesia 32: 163-169.
- Ravensroft PJ (1978) Simple mandatory minute volume. Anaesthesia 33: 246-249.
- Tehrani FT (2005) The origin of adaptive support ventilation. Int J Artif Organs 28: 1051-1052.
- Mireles-Cabodevila E, Diaz-Guzman E, Heresi GA, Chatburn RL (2009) Alternative modes of mechanical ventilation: A review for the hospitalist. Cleve Clin J Med 76: 417-430.
- Otis AB, Fenn WO, Rahn H (1950) Mechanics of breathing in man. J Appl Physiol 2: 592-607.
- Veelo DP, Dongelmans DA, Binnekade JM, Paulus F, Schultz MJ (2010) Adaptive support ventilation: A translational study evaluating the size of delivered tidal volumes. Int J Artif Organs 33: 302-309.
- Sulemanji D, Marchese A, Garbarini P, Wysocki M, Kacmarek RM (2009) Adaptive support ventilation-An appropriate mechanical ventilation strategy for acute respiratory distress syndrome? Anesthesiology 111: 863-870.
- Laubscher TP, Frutiger A, Fanconi S, Jutzi H, Brunner JX (1994) Automatic selection of tidal volume, respiratory frequency and minute ventilation in intubated ICU patients as startup procedure for closed-loop controlled ventilation. Int J Clin Monit Comput 11: 19-30.
- Laubscher TP, Heinrichs W, Weiler N, Hartmann G, Brunner JX (1994) An adaptive lung ventilation controller. IEEE Trans Biomed Eng 41: 51-59.
- Arnal JM, Wysocki M, Nafati C, Donati S, Granier I, et al. (2008) Automatic selection of breathing pattern using adaptive support ventilation. Intens Care Med 34: 75-81.
- https://www.hamilton-medical.com/Solutions/Adaptive-Support-Ventilation-ASV.html
- Morato JB, Mayara TAS, Juliana CF, Pedro C (2012) comparison of 3 modes of automated weaning from mechanical ventilation: a bench study J Crit Care 27: 741.e1-741.e8.
- Zhu F, Gomersall CD, Ng SK, Underwood MJ, Lee MA (2015) A randomized controlled trial of adaptive support ventilation mode to wean patients after fast-track cardiac valvular surgery. Anesthesiology 122: 832-840.
- Mohamed KAE, Maraghi SKE (2014) Role of adaptive support ventilation in COPD patients. The Egyptian Society of Chest Diseases and Tuberculosis 63: 449-454.
- Arna JM, Garnero A, Novonti D, Demory D (2013) Feasibility study on full closed-loop control ventilation (IntelliVent-ASV) in ICU patients with acute respiratory failure: a prospective observational comparative study. Critical Care 17: R196.
- Elmorsy AA, Beshay BN, Mousa EH (2015) Adaptive support ventilation versus biphasic positive airway pressure in patients with acute exacerbation of chronic obstructive pulmonary disease. Research and Opinion in Anesthesia & Intensive Care 2: 34-42.
- Chen CW, Wu CP, Dai YL, Perng WC, Chian CF, et al. (2011) Effects of implementing adaptive support ventilation in a medical intensive care unit. Respir Care 56: 976-983.
- Cabodevila EM, Diaz-Guzman E, Arroliga AC, Chatburn RL (2012) Human versus computer controlled selection of ventilator settings: An evaluation of adaptive support ventilation and mid-frequency ventilation. Critical Care Research and Practice.
- Gruber PC, Gomersall CD, Leung P, Joynt GM, Ng SK, et al. (2008) Randomized controlled trial comparing adaptive-support ventilation with pressure-regulated volume-controlled ventilation with automode in weaning patients after cardiac surgery. Anesthesiology 109: 81-87.
- Sviri S, Bayya A, Levin PD, Khalaila R, Stav I, et al. (2012) Intellivent ventilation in the intensive care unit. Crit Care 28: 6-12.
- Agarwal R, Srinivasan A, Aggarwal AN, Gupta D (2013) Adaptive support ventilation for complete ventilatory support in acute respiratory distress syndrome. Respirology 8: 1108-1115.

Open Access Journals
- Aquaculture & Veterinary Science
- Chemistry & Chemical Sciences
- Clinical Sciences
- Engineering
- General Science
- Genetics & Molecular Biology
- Health Care & Nursing
- Immunology & Microbiology
- Materials Science
- Mathematics & Physics
- Medical Sciences
- Neurology & Psychiatry
- Oncology & Cancer Science
- Pharmaceutical Sciences