













 55 / 65
55 / 65

Page 79
May 24-25, 2018
London, UK
Vascular Surgery 2018
3
rd
Edition of World Congress & Exhibition on
Vascular Surgery
Journal of Vascular and Endovascular Therapy
ISSN: 2573-4482
Introduction:
Isolated abdominal aortic dissection (IAAD) refers
to aortic dissection (AD) inferior to the diaphragm, which is
very rare. Marfan syndrome (MFS) is an autosomal dominant
connective tissue disorder, which is mostly presented as garlic-
like aortic aneurysm in cardiovascular system. To the best of our
knowledge, no such a case concerning MFS presented as IAAD
has been reported before.
Case Report:
A 37-year-old femalewith no history of hypertension
was referred to our hospital for chest tightness. She had been
initially diagnosed as spontaneous IAAD one month before with
successful analgesic and antihypertensive treatment at a local
hospital. On physical examination, the patient’s blood pressure
was 138/80 mmHg. Laboratory tests showed D-dimer of 2.13 ug/
ml (<0.5 ug/ml), FDP of 8.42 ug/ml (0-5 ug/ml). Echocardiography
revealed severe aortic regurgitation. CT showed an obvious
compression of the left atrium by asymmetrical dilatation of non-
coronary sinus. Abdominal aortic dissection originated distally
to the superior mesenteric artery (SMA) ostium and extended
downward to the bilateral common internal iliac artery. Then
FBN1 mutation was found by gene analysis, thus the diagnosis of
Marfan syndrome (MFS) was confirmed. She underwent Bentall
procedure only and discharged on calcium channel blocker
and warfarin. On follow-up at 1 year, the patient was doing well
physically. CT scanning found no obvious extension of IAAD or
aortic growth in diameter.
Lessons:
First, this is the first case report of MFS combined with
both asymmetrical aortic root aneurysm and spontaneous IAAD,
which enriches our understanding of the clinical manifestations
of MFS. Second, we should take aorta as a whole organ in which
multiple levels of lesions may occur simultaneously, so it is
necessary to assess the whole aorta in order to prevent serious
missed diagnosis. Third, for MFS patient with IAAD, conservative
treatment under careful surveillance seems satisfactory on a
short-term follow up. Further follow-up is still needed to confirm
the long-term effect.
Recent Publications
1. Cheng L, Huang F, ChangQ, Zhu J, Yu C, Liu Y, et al. (2010)
Repair of extensive thoracoabdominal aortic aneurysm
with a tetrafurcate graft: midterm results of 63 cases.
The Heart Surgery Forum 13(1):E1-6.
2. Sun X, Zhang L, Yu C, Qian X and Chang Q (2014)
One-stage repair of extensive aortic aneurysms: mid-
term results with total or subtotal aortic replacement.
Interactive Cardiovascular &Thoracic Surgery 18(3):278-
82.
3. Zhang L, Yu C, Qian C, Luo X, Qiu J and Liu S (2016)
Comparison of gene expression profiles in aortic
dissection and normal human aortic tissues. Biomedical
Reports 5(4):421-7.
4. Liu P, Qian C, Qian X, Sun X, Yu C, Tian C, et al. (2016)
Early and mid-term results after hybrid total arch repair
of DeBakey type I dissection without deep hypothermic
circulatory arrest. Interactive Cardiovascular & Thoracic
Surgery 23(4):608.
Biography
Cun Tao Yu is one of the most famous cardiovascular surgeons in China.
He is especially good at all kinds of operation of large vessels and has com-
pleted over 1500 operations such as total arch replacement and thoracoab-
dominal aortic replacement. Jin Lin Wu is his doctoral candidate.
jinlinhorsy@outlook.comMarfan syndrome presented as asymmetrical aortic root
aneurysm and spontaneous isolated aortic abdominal dissection
Jin Lin Wu
and
Cun Tao Yu
Peking Union Medical College(PUMC), China
Jin Lin Wu et al., J Vasc Endovasc Therapy 2018, Volume 3
DOI: 10.21767/2573-4482-C1-002
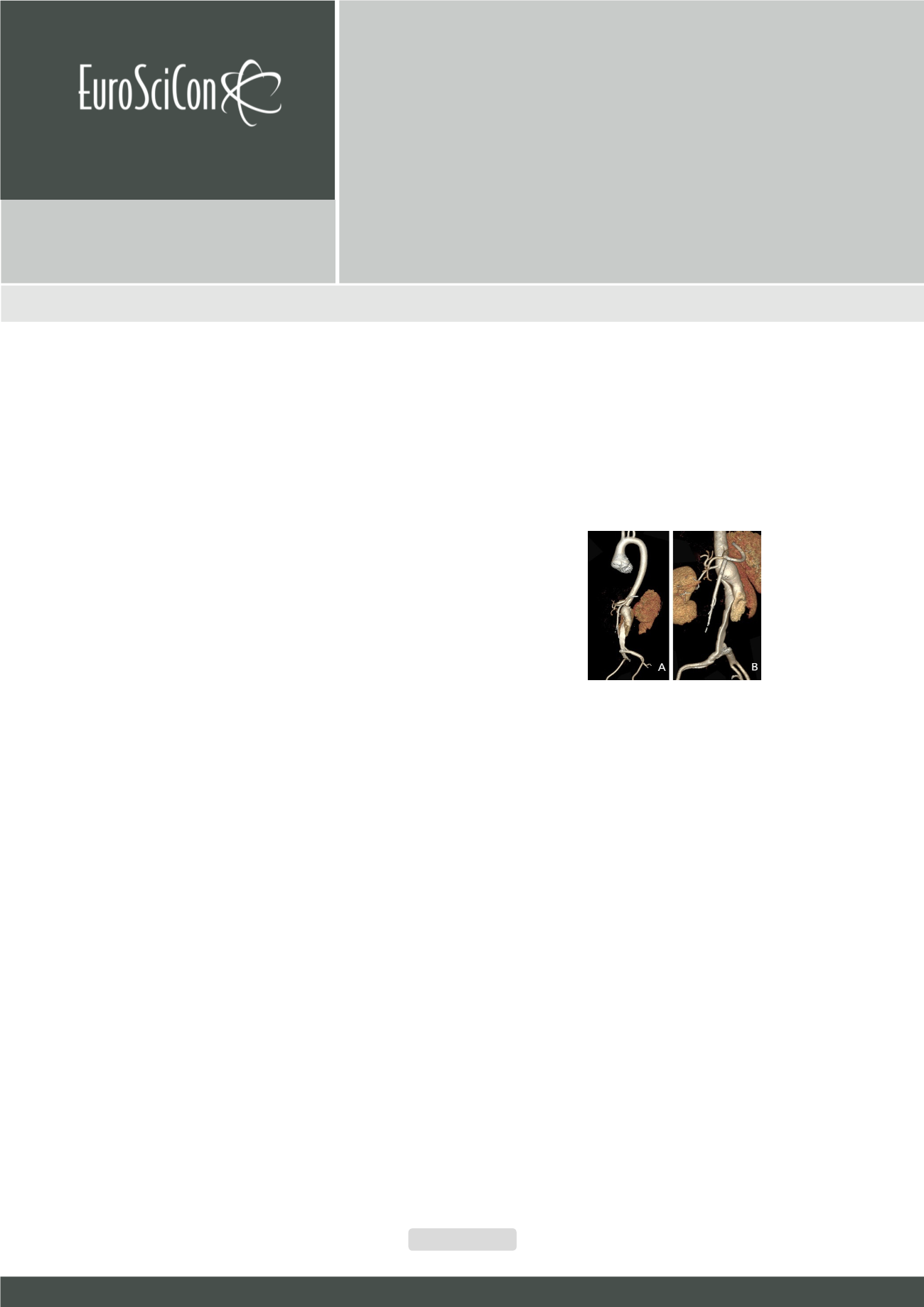
Figure 1:
A: 3-D re-construction of CT scanning of the whole aorta. B: 3-D
re-construction of CT scanning of the abdominal aorta.