













 11 / 20
11 / 20

Page 35
Journal of Medical Physics and Applied Sciences
ISSN: 2574-285X
I n t e r n a t i o n a l C o n f e r e n c e o n
Nuclear Medicine &
Radiation Therapy
Nuclear Medicine & Radiation Therapy 2018
O c t o b e r 0 1 - 0 2 , 2 0 1 8
S t o c k h o l m , S w e d e n
Combining IMRT and DIBH for the treatment of mediastinal
lymphomas: what’s the benefit?
Joao Antonio Maia Garcia Fonseca, N Ferreira, R Colaco, A
Mota, D Braga, J Silvestre, L Afonso, M Sousa, T Madaleno, L
Mirones, I Antao and F Santos
Instituto Portugues de Oncologia de Lisboa Francisco Gentil (IPOLFG), Portugal
Joao Antonio Maia Garcia Fonseca et al., J. med phys & appl sci 2018, Volume: 3
DOI: 10.21767/2574-285X-C1-002
Background:
Radiotherapy plays an important role in the treatment of Hodgkin lymphoma (HL). However, long term survivors treated
with mediastinal RT have an increased risk for the development of cardiovascular disease and secondary cancers. Efforts have been
made to reduce the rates of late toxicity and promising results have been published with intensity modulated radiation therapy (IMRT)
and deep inspiration breath-hold (DIBH). Patients with HL are often young with good respiratory function, enabling the use of DIBH.
Objective:
To evaluate the potential benefit of combining IMRT with DIBH to decrease cardiac and lung dose in mediastinal RT.
Material & Methods:
Three patients with cervical and mediastinal lymphoma involvement received involved site radiotherapy (ISRT)
with 30 Gy in 15 fractions. Each patient underwent a planning CT scan in free-breathing (FB) and DIBH using a 5 point thermoplastic
mask. IMRT plans for FB and DIBH were created and compared with respect to PTV coverage and doses to organs at risk.
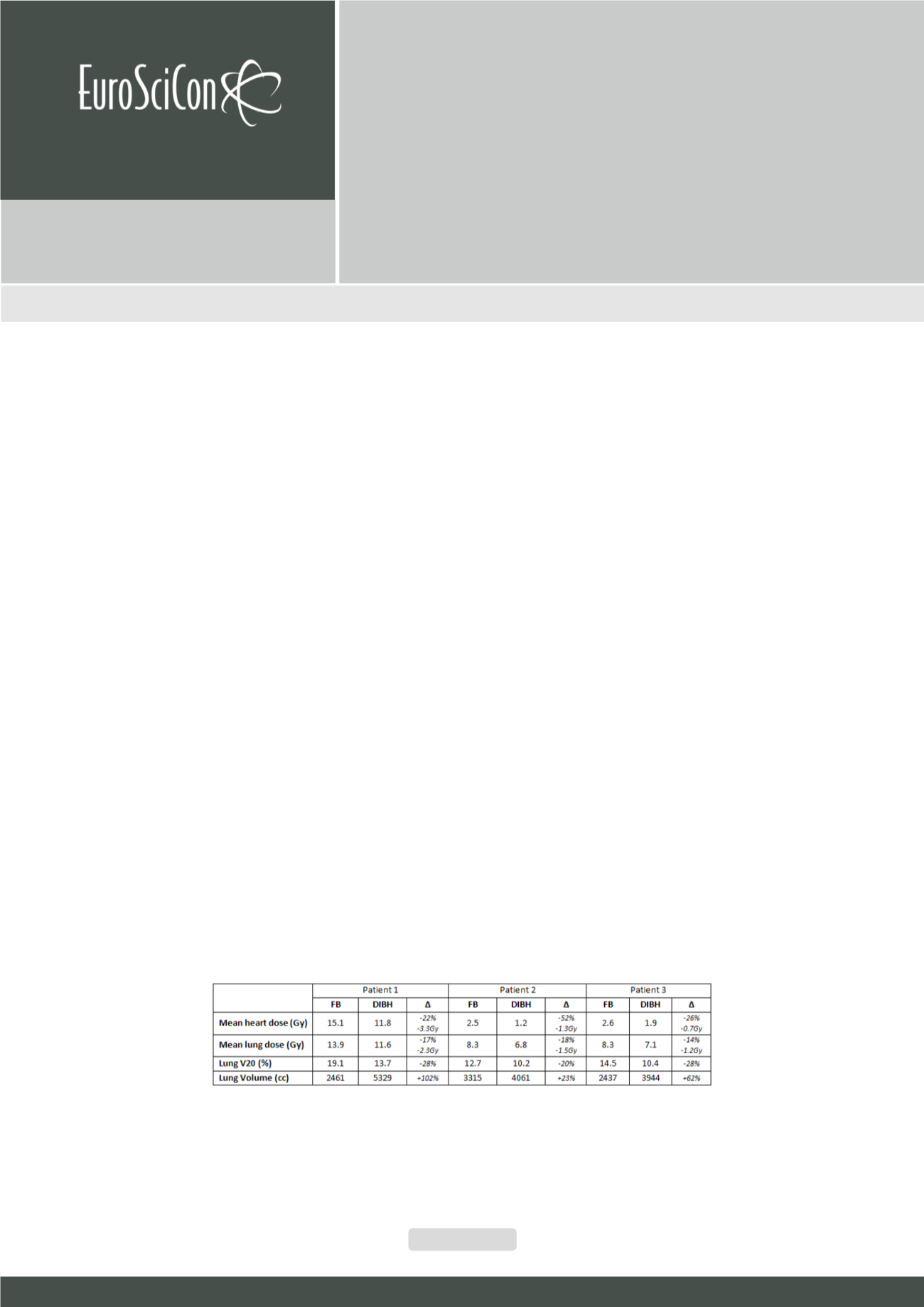
Results:
Patient 1 had a large PTV volume extending downwards into the anterior mediastinum reaching the cardiofrenic space while
patients 2 and 3 had disease only on the upper mediastinum. Mean heart dose was lower with DIBH in all patients (~22-52%). Greater
lung expansion was achieved with DIBH which contributed to lower mean lung doses (~14-18%) and lung V20 (~20-28%). Higher
absolute decreases on mean heart and lung doses were seen on patient 1. PTV coverage (D95, V95) was similar for both plans in all
patients. DIBH-IMRT was chosen for treatment delivery on patients 1 and 2.
Discussion:
Significant decreases on heart and lung doses can be achieved while not comprising PTV coverage. Patient anatomy and
disease extension will determine the degree of dosimetric improvement when using DIBH. Also, appropriate patient compliance is
essential to perform DIBH.
Conclusion:
Combining DIBH and IMRT can significantly improve doses on heart and lung when using mediastinal RT and thus reduce
long-termmorbidity. Choice between treatment delivery techniques should be made on an individualized basis.
Biography
João António Maia Garcia Fonseca is a Medical Doctor and has completed his studies in Nova Medical School Lisbon in 2014. He is currently in his last year of Residency in
Radiation Oncology at Instituto Português de Oncologia de Lisboa which began in 2015. Over the past years, he has presented several posters and oral communications in both
national and international conferences. In 2018, he presented poster in ESTRO 37 and 20th ESMO World Gastrointestinal Congress.
jgarciafonseca@gmail.com jfonseca@ipolisboa.min-saude.pt