Keywords
Orthodontic patients; Dental practice; Social factors
Introduction
According to the literature review, the incidence of orthodontic anomalies and deformities is too high, and many children and parents are looking for orthodontist to solve serious functional and aesthetic problems. Most often, they see their problem too late and cannot be treated with anything other than fixed technique. And this is a problem, not for other reasons, but because the fixed orthodontic treatment is too expensive and most of the parents cannot afford it. Unfortunately, the general practitioner dentist who is uncompetitive with regard to orthodontic malocclusions is also actively involved in this process.
By the Bulgarian orthodontist’s opinion, work, motivation and discussion of problems with the patient and his / her parents will lead to raising the level of patient's health intelligence and will place high demands on their treatment [1].
On the other hand, world orthodontic literature lays down the 21st century as a century of aging orthodontics. This is due to new innovative treatment techniques as well as to demographic changes with the average age patients, which is increasing worldwide [2].
A serious discussion sets out the factors that can contribute to disturbing normal physician-patient relationships. Several are the main theories that discuss the success of orthodontic treatment:
1. Health culture and patient’s awareness;
2. Current knowledge and competence of the dental practitioners, about the modern methods of treatment with fixed orthodontic appliances; Active prophylactic examinations for the detection of orthodontic malocclusions. According to a lot of Bulgarian orthodontists, this check - up is purposeful [1,3];
3. Inequality of access and quality of orthodontic services [1,4].
Providing information is an essential part of healthcare. Studies by leading Bulgarian researchers show that the dentist takes a substantial part in the patient's health education. According to them, the following basic principles are laid down in health education:
1. Social orientation - health behavior is formed with the patient by revealing the social determinants of health and illness;
2. Mass - health education must reach to all into society and is the basis of dental practitioner’s behavior;
3. Popularity - the language of communication between orthodontist and the patient should be understandable;
4. Scientific - health education must be scientifically based;
5. Accuracy - patient’s awareness should address current health problems;
6. Concurrency - combining important health issues for the patient;
7. Emotionality - health education must cause emotions in the patient; to induce a need for change in health behavior;
8. Optimism - if the treatment is started in a timely manner and is conducted systematically, optimal results for the patient will be achieved;
9. Focus - health education is an integral part of prevention and prophylaxis. It creates health knowledge, habits and skills to strengthen the physical and psychological resistance of the body;
10. Systematicity, continuity and consistency - the formation of a health culture is a complex and prolonged process that requires continuous actions in health education [1,3].
Methods of health awareness are limited to the following groups
• Methods with predominance of oral speech;
• Methods with predominance of the printed word;
• Methods with predominance of visual elements;
• Combined methods [4-6].
Data in the literature suggests that in the recent years, patients often use the internet to supplement their awareness. The information in the media may be inaccurate, misleading or inappropriate. Scientists are supposed to provide reliable and relevant sites for targeting relevant Internet sources. Discussion of problems in Internet forums, additional information, second opinion or support is a very small part of the possibilities of the Internet. People often seek confirmation that the right decision was made even by strangers just because they were subjected to the same treatment [7,8].
Materials and Methods
Personal questionnaire has been composed based on the literature review for the pilot study of parents (n=50). The inquiry card consists of 36 questions (open, closed and mixed):
1. Socio-demographic characteristics;
2. The role of the medical school and general practitioners;
3. Parents attitudes for orthodontic treatments;
4. Awareness for orthodontic treatment;
5. Financing tools of orthodontic treatment.
Most studies over subjective experiences of patients in orthodontic treatment have been conducted using questionnaires to assess oral health and anxiety - SF-36, MHI-5, CHQ-12 [3,9].
Epidemiological method
In this study we have used a descriptive epidemiology and a cross-sectional design to determine the health awareness of parents under the influence of various external factors. The individual characteristics and material and educational status have been taken into account for the parents. The collected data have allowed finding out whether awareness is changing under the influence from family, school or dentists.
Sociological method
Survey method interview: Sociological information is collected by conducting a standard individual interview and direct individual questionnaire for parents. In this study, we have been used the following indices:
• VAS (Visual Analogue Scale);
• IOTN (Index of Orthodontic Treatment Need) [3,7]. The IOTN index, known and applicable in other countries, has been validated by a Bulgarian orthodontist Petrunov V. to carry out epidemiological data of tooth-jaws deformities and to improve the oral health status of children in the country [3].
Documentary method: For the purpose of the scientific study, data from Regional Health Inspectorate - Plovdiv have been used about the number of dentists distributed in the respective practices and centers.
Statistical method
The data have been processed using specialized statistical product IBM SPSS 19.0 for Windows. It has been applied to the following statistical analysis:
• Analysis of the frequency distribution;
• Nonparametric analysis - to assess the hypotheses (criterion of Pearson agreement);
• Regression analysis - α-factor Kronbach;
• Graphical analysis - results has been performed in EXCEL 2007.
A sample of 259 patients who received orthodontic treatment completed a questionnaire. The average age of children is 12.56 ± 3.14 years, respectively 12.38 ± 3.22 for boys and 12.69 ± 3.07 for girls, P> 0.05. Socio-demographic characteristics of children are presented on Table 1:
Table 1 Age-gender distribution.
| Age (years) |
Gender |
Total |
% |
Sp |
| Boys (n) |
% |
Sp |
Girls (n) |
% |
Sp |
| 7 |
6 |
5.00 |
1.99 |
5 |
3.68 |
1.61 |
11 |
4.26 |
1.26 |
| 8 |
7 |
5.83 |
2.14 |
5 |
3.68 |
1.61 |
12 |
4.65 |
1.31 |
| 9 |
18 |
15.00 |
3.26 |
14 |
10.29 |
2.61 |
32 |
12.40 |
2.05 |
| 10 |
17 |
14.17 |
3.18 |
21 |
15.44 |
3.10 |
38 |
14.73 |
2.21 |
| 11 |
7 |
5.30 |
2.14 |
13 |
9.56 |
2.52 |
20 |
7.75 |
1.66 |
| 12 |
1 |
0.83 |
0.83 |
9 |
6.52 |
2.10 |
10 |
3.88 |
1.20 |
| 13 |
7 |
5.83 |
2.14 |
4 |
2.90 |
1.43 |
12 |
4.26 |
1.26 |
| 14 |
17 |
14.17 |
3.18 |
19 |
13.97 |
2.97 |
36 |
13.95 |
2.16 |
| 15 |
20 |
16.67 |
3.40 |
20 |
13.97 |
2.97 |
40 |
15.12 |
2.23 |
| 16 |
8 |
6.67 |
2.28 |
14 |
10.29 |
2.61 |
22 |
8.53 |
1.74 |
| 17 |
6 |
5.00 |
1.99 |
8 |
5.88 |
2.02 |
14 |
5.43 |
1.41 |
| 18 |
6 |
5.00 |
1.99 |
7 |
4.41 |
1.76 |
13 |
4.65 |
1.31 |
| Total |
121 |
46.72 |
3.11 |
138 |
53.28 |
3.11 |
259 |
100.00 |
- |
Table 1 gives information on the gender and age of the children who participated in the study, allocated for each year from 7 to 18 years. There is also a distribution of the relative proportions by gender for the children: 53.28 ± 3.11% are girls and 46.72 ± 3.11% - boys.
The highest relative share in girls was observed in the age of 10 years (15.44 ± 3.1%), for boys this was 15 years of age (16.67 ± 3.4%), P <0.05 (χ2 = 12.22). This result allows age and gender to be commented on as factors that are relevant to meeting the optimal deadlines for orthodontic treatment.
Results
The conditions that form an optimal physician-patient relationship are a lot. In modern dental practice, putting the abstract framework of ethical principles helps to achieve basic relationships with patients. Dental doctors, in order to be competitive on the market, must offer highly specialized services and not just to help the patient, but also to be able to keep their tone and their wonderful mood, despite the fact that they are overwhelmed. Fatigue is a natural consequence of the overcompetency of the orthodontist. Therefore, however strange it may seem, for the optimal physician-patient relationship, the greatest contribution to dental practice brings the investment into quality staff [10,11].
In the second question from children’s questionnaire “Do you like to visit the dentist?” the following results are presented at Table 2:
Table 2 Opinion of the children who answered the question "Do you like to visit your dentist?"
| Gender |
Wish to visit dentist |
Without wish |
Can’t decide |
Total |
| n |
% |
Sp |
n |
% |
Sp |
n |
% |
Sp |
n |
% |
Sp |
| Boys |
65 |
25.19 |
2.70 |
41 |
15.89 |
2.28 |
15 |
5.81 |
1.46 |
121 |
46.90 |
3.11 |
| Girls |
51 |
19.77 |
2.48 |
70 |
27.13 |
2.77 |
16 |
6.20 |
1.46 |
137 |
53.10 |
3.11 |
| Total |
116 |
44.96 |
- |
111 |
43.02 |
- |
31 |
12.02 |
- |
258 |
100.0 |
- |
The typical characteristics of dental practice are to achieve a clinical outcome (positive) for the patient, to optimize aesthetics and personal satisfaction with the work done by the doctor. The first two quality features relate to patients, and the third one is very important to the dentist.
Workplace relationships that affect patients can also determine the attitude of the patient with whom he attends dental practice. From Table 2 it is clear that when the attitude of visit is related to the parent's expressed and discussed fear, this further exacerbates the negative expectations of the child itself [12-14].
The patient’s motivation to advertise and refer doctor to his friends is perhaps the most essential in terms of satisfaction with the results achieved. Trust is very difficult to achieve and is easily lost and how to build it when patient relationships include payment of dental services [13].
In most countries, the payment of orthodontic services is a normal practice, not surprising for the patient. In Bulgaria, after the collapse of communism and the introduction of market relations, dentists were placed in a situation that demanded pay (too high for the standards at that time) and consequently led to the open dissatisfaction of the patients. In their (patients) protection is necessary to comment fact that the whole population of the country did not pay for any health services for 45 years. On the other hand, the dentist leaves the impression into society that with the smile, the friendly appearance, the clean clothes, and above all - the ease with which he works, wants too much money for healing. Thus, in society becomes mostly negative attitude stowards the personality of the dentist, who such performs a highly specialized activity and he does his jobs as well.
Against the backdrop of these attitudes towards the dental profession, the patient is highly valued to keep the time the dentist spends to educate and promote oral hygiene and eating habits. Ethical relationships become a first class when the patient understands that the dentist seeks to guide him with all his behavior to the prevention and prophylaxis of oral diseases rather than for higher payment.
Therefore, family-based health habits have a definite impact on the child's understanding of the need for visits to the dental office. The responsibility of parents is high, both in educating hygienic habits and in forming a friendly attitude towards the dentist. The personal example is perceived unconditionally, and the preliminary conversation in the family is of utmost importance when discussing the child's consent for the upcoming treatment at Figure 1. are presented the distribution of data for children which answered the question “Do you trust your dentist?”. The graphic shows also their distribution per age from 7 to 18 years:
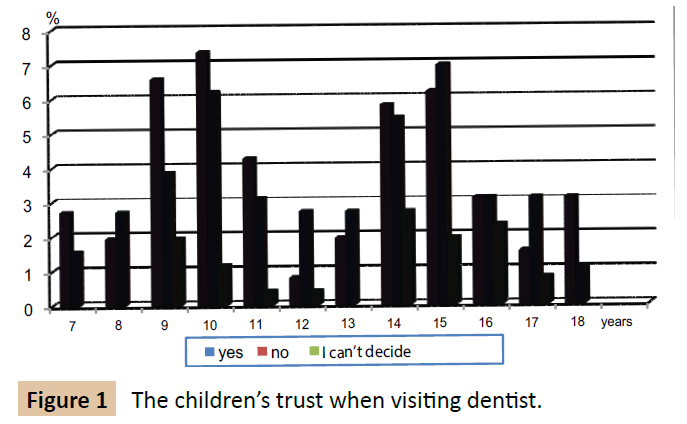
Figure 1: The children’s trust when visiting dentist.
The data presented at Figure 1 shows that children who wish and trust their dentist are 44.62 ± 3.08%. According to literature data, the parents of these children accept calmly and confidently dental treatment. In addition, however, other oral health researchers have sought a specific link between the orthodontic past of parents and child motivation in the orthodontic treatment [2,7,13]. This concept was introduced for the first time in 1968 by Lewit & Virolinen.
On particular interest are the results where it conceals the idea of improving oral health through self-regulating behaviors. And for the present study, the self-assessment of the child is very important. There are distinct views in the literature that personal example given by the dentist is very important recent days [1,4,10,15]. It’s important because the doctor can educate behavioral, hygienic, educational, and other habits in their patients.
Conclusion
For the optimal physician-patient relationship, the greatest contribution to dental practice brings the investment into quality staff.
The typical characteristics of dental practice are to achieve a clinical outcome (positive) for the patient, to optimize aesthetics and personal satisfaction with the work done by the doctor.
The patient’s motivation to advertise and refer doctor to his friends is perhaps the most essential in terms of satisfaction with the results achieved. There should be no question that referrals are the lifeblood of the orthodontic practice. That’s why the respect and honest approach to the patient is from the first necessity. The challenge is how to keep the best patientphysician relationships when the practice?
References
- Borzabadi-Farahani A (2011) An insight into four orthodontic treatment need indices. Prog Orthod 12: 132-142.
- Kokich VG (1993) Anterior dental esthetics: An orthodontic perspective. I. Crown Length. J Esthet Dent 5: 19-23.
- Krumova V, Petrunov V, Gurgurieva V (2007) Aesthetic analysis of the soft tissue profile and the position of the incisors in relation to the aesthetic horizontal line. Balkan Orthodontic symposium-Sofia, Orthodontics Review 9: 18.
- Badri P, Saltaji H, Flores-Mir C (2014) Factors affecting children's adherence to regular dental attendance: A systematic review. J of Am D Assoc 145: 817-828.
- Ackerman MB, Thornton B (2011) Post treatment compliance with removable maxillary retention in a teen age population: A short-term randomized clinical trial. Orthodontics 12: 22-27.
- Al-Omiri M, Alhaija E (2006) Factors affecting patient satisfaction after orthodontic treatment. Angle Orthod 76: 422-431.
- Shaw WC (1981) Factors influencing the desire for orthodontic treatment. Eur J Orthod 3: 151-162.
- Vodopivec-Jamsek V, de Jongh T, Gurol-UrganciI, Atun R, Car J (2012) Mobile phone messaging for preventive health care. Cochrane Database Syst Rev 12: CD007457.
- Keles F, Bos A (2013) Satisfaction with orthodontic treatment. Angle Orthod 83: 507-511.
- Eppright M, Shroff B, Best AM, Barcoma E, Lindauer SJ (2014) Influence of active reminders on oral hygiene compliance in orthodontic patients. Angle Orthod 84: 208-213.
- Johal A, Alyaqoobi I, Patel R, Cox S (2015) The impact of orthodontic treatment on quality of life and self-esteem in adult patients. Eur J Orthod 37: 233-237.
- Dinkova M (2013) Orthodontic treatment management in adult patients with periodontal diseases. Sofia, Pp: 45-49.
- Pratt MC, Kluemper GT, Lindstrom AF (2011) Patient compliance with orthodontic retainers in the post retention phase. Am J Orthod Dentofacial Orthop 140: 196-201.
- Schott TC, Schlipf C, Glasl B, Schwarzer CL, Weber J, et al. (2013) Quantification of patient compliance with Hawley retainers and removable functional appliances during the retention phase. Am J Orthod Dentofacial Orthop 144: 533?540.
- Armstrong AW, Watson AJ, Makredes M, Frangos JE, Kimball AB, et al. (2009) Text-message reminders to improve sunscreen use: A randomized, controlled trial using electronic monitoring. Arch Dermatol 145: 1230-1236.