Keywords
Osteoporosis; Aortic; Vascular; Calcification
Introduction
Cardiovascular disease (CVD) continues to be the leading cause of mortality in post-menopausal women and the identification of those at risk of CVD and subsequent CV events has relied on the assessment of traditional clinical risk factors such as hypertension, obesity, smoking status, family history and diabetes mellitus [1]. Moreover, abdominal aortic calcification (AAC), a marker of subclinical atherosclerosis, is a predictor of subsequent CV-associated morbidity and mortality [2-5]. Computed tomography (CT) is recognised as the ‘gold-standard’ method for the quantitative assessment of calcification with relatively good precision and accuracy [6-11], however, much of the data available has been limited to measurements of coronary calcification [7,11] and to high risk populations such as those with Chronic Kidney Disease (CKD) [6,7-9]. Furthermore, the method is limited by high radiation exposure and cost [10-12].
Lateral vertebral fracture assessment (VFA) imaging has been shown to be a reasonable substitute for standard radiography to detect vertebral deformities, and can be readily performed at the time of bone densitometry with minimal additional time and radiation exposure [13-15]. The abdominal aorta (AA) can be visualized on lateral VFA scan images anterior to the lumbar spine, and the use of lateral VFA has been proposed as a useful imaging tool for the semi-quantitative assessment of AAC [16], with reasonably good sensitivity and specificity when compared to conventional radiographs [17]. Previous assessments of the accuracy of lateral VFA scans for quantifying AAC by comparison with the gold-standard of CT have reported good sensitivity of lateral VFA for the assessment of AAC with results closely comparable to that of CT; suggesting that lateral VFA scans may allow concurrent assessment of AAC as well as bone mineral density (BMD) in women referred for routine screening for low BMD and osteoporosis [6]. However, studies have been limited to high risk populations with a high incidence and extent of VC [6,9].
Pulse wave velocity (PWV) is a simple, non-invasive method of measuring arterial stiffness which has been shown to be an independent predictor of CV-related events and mortality [18-24]. PWV is in part dependent on the atherosclerotic burden and/ or medial calcification and is widely used in the fields of renal and diabetic research. PWV provides an alternative method for estimating AC, hence the rationale for its inclusion in this study. This study aims to assess whether lateral VFA scan images can be used to detect AAC as determined by the gold-standard of CT in a lower risk population.
Materials and Methods
Subjects
Four hundred and forty-four healthy ambulatory postmenopausal women, mean age of 62 (6.4) years were recruited from the Osteoporosis Unit at Guy's Hospital following referral by primary care physicians for assessment of their bone mineral density (BMD) by dual energy x-ray absorptiometry (DXA) and as part of a PhD research program. Each participant gave informed consent and the study was conducted in accordance with the ethical standards of the Research and Ethics Committee of Guy's and St Thomas' NHS Foundation Trust. All participants were seen in the Osteoporosis Unit and completed questionnaires which recorded information relating to smoking habits, alcohol intake, previous fractures, history of con-medications, and presence of CV risk factors including family history of CV disease, history of hypertension, hypercholesterolemia and diabetes mellitus. The following study procedures were performed on the subjects: carotid to femoral PWV ultrasound measurements to assess aortic stiffness, CT scans of the chest and abdomen, and lateral VFA scans to quantify AAC.
Quantitative assessment of VC Using CT
A sub-group consisting of one hundred and thirteen subjects underwent non-contrast non-diagnostic, un-gated CT scans of the chest and abdomen. The scans were performed using the Philips Precedence 16-slice SPECT/CT helical scanner (Philips Healthcare, Best, Netherlands). The scan field of view (FoV) was approximately 50cm and included the iliac arteries, abdominal aorta, thoracic aorta and carotid arteries. Scan images were reconstructed into contiguous 3mm transverse images for viewing on an image analysis workstation. All scan images were viewed and analysed using the semi-automated hybrid viewer function on Hermes Gold™ imaging software. Abdominal aortic calcification was evaluated using CT scans for direct comparison to AAC as measured using lateral VFA scans. Vascular calcification was also assessed at other vascular sites included during the CT scan acquisition. Scans were assessed by one clinical scientist (SE), blinded to subject demographics, BMD results and lateral VFA AAC scores. Each 3 mm transverse image was analysed individually and calcified deposits were defined as any area greater than 1 mm2 within the blood vessel 5 being assessed with a HU of ≥ 130. The previously described total Agatston [25,26], modified Agatston [27] and volume score [28] were obtained by summing the scores for all cross-sectional images.
Semi-quantitative assessment of AAC using lateral VFA imaging
Four hundred and forty-four subjects had lateral single-energy VFA (IVA-HD) scans of the lumbar spine performed using the Hologic Discovery QDR 4500 densitometer (Hologic, Bedford MA). Scans were obtained using an established local protocol for lateral VFA scan acquisition which was modified to include the lumbar region only using a rotating C-arm which required the subject to lie supine with arms raised. One hundred and four (31%) of the 444 scans could not be evaluated due to poor image quality primarily as a result of abdominal obesity or overlying bowel gas obscuring the walls of the AA. Abdominal aortic calcification was assessed on the lateral VFA scan images by a clinical scientist (SE), blinded to subject demographics and BMD results with scans identified only by the subject’s study number. Scans were analyzed using both the semi-quantitative 24-point and 8-point scoring methods in which both the location and the extent of calcification at each lumbar vertebral segment (L1-L4) were evaluated [16].
Measurement of vascular stiffness
Four hundred and forty-four subjects had carotid to femoral artery PWV performed using the SphygmoCor (AtCor Medical LTD, Australia) PWV system. Measurements were made by one clinical scientist (SE), and any readings which did not conform to the internal quality checks provided by the SphygmoCor software were rejected and subsequently repeated. Measurements were made in triplicate, with mean PWV values used for data analysis. Measurements of PWV were not obtained for 82 (19%) of the total study cohort of 444 subjects, primarily as a result of excessive amounts of adipose tissue at the femoral artery measurement site precluding an accurate recording of the pressure pulse. The validation of this method and its reproducibility has been previously described with intra- and inter-observer repeatability coefficients of 0.935 m/s and 0.890 m/s respectively [29].
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics version 20 and MATLAB. Study population characteristics are presented as the mean and standard deviation (SD) unless otherwise stated. The student’s t-test and chi-squared test were used to test for significant differences in characteristics between subject groups for PWV and lateral VFA. The Kolmogorov-Smirnov test was used to assess normality of distribution of measures of VC including lateral VFA AAC scores, CT VC scores and PWV. Pearson’s correlation coefficient was calculated to assess the correlation between lateral VFA and CT AAC scores and the correlation between PWV and calcium scores obtained using lateral VFA and CT. The sensitivity, specificity, positive predictive value (PPV) and negative predictive values (NPV) were calculated for the 24-point lateral VFA scoring method for identifying calcium detected by CT with a binary cut-off of 0 for zero calcium and 1 for calcium present. To allow an assessment of whether the accuracy of lateral VFA changes with increasing severity of AAC on CT, sensitivity, specificity, PPV and NPV were calculated for tertiles of CT calcium score for the AA with thresholds set at ≥ 117AU, ≥ 670 AU for the Agatston score, ≥ 2161.9 AU, ≥ 15304.4AU for the modified Agatston score and ≥ 0.074 cm3 and ≥ 0.335 cm3 for the volume score. Unlike coronary calcium scores which have established cut-points that are associated with increased CV disease incidence; all CT scores at the AA in this study were divided into equal tertiles as no established cut-off points exist for AAC. The area under the curve (AUC) was calculated using receiver operating characteristic (ROC) analysis. Multi-linear regression analysis was used to assess associations between PWV with AAC as measured by lateral VFA and VC measured using CT at multiple vascular sites, correcting for confounders associated with PWV and/or VC. Confounding variables included age, BMI, MAP, antihypertension medication and smoking status. A p-value of <0.05 (95% CI) was accepted as statistically significant.
Results
Subjects had a mean age of 62 years (range 50 to 81). Fifty-five per cent (n=244) of subjects had a family history of CV disease and 13% (n=58) had confirmed hypertension with 10% (n=44) taking antihypertensive medication (Table 1).
Table 1 Summary of study group characteristics.
| n=444 |
Mean (SD) |
| Age (years) |
61.7 (6.4) |
| Height (m) |
1.62 (0.07) |
| Weight (kg) |
65.8 (12.0) |
| BMI (kg/m2) |
24.9 (4.4) |
| Total cholesterol (mmol/l) |
6.0 (0.9) |
| Total triglycerides (mmol/l) |
1.0 (0.4) |
| HDL-cholesterol (mmol/l) |
2.0 (0.5) |
| LDL-cholesterol (mmol/l) |
3.5 (0.8) |
| Mean arterial pressure (mm Hg) |
93.6 (10.0) |
| PWV (m/s) |
8.9 (1.7) |
| Lumbar spine T-score |
-1.3 (1.2) |
| Total hip T-score |
-0.8 (0.9) |
| Hip neck T-score |
-1.2 (0.9) |
| Family history CVD (%) |
55 |
| Hypertension (%) |
13 |
| Hypertension treatment (%) |
10 |
| History of fracture (%) |
31 |
| Current Smoker (%) |
Relationship between lateral VFA and CT
Abdominal aortic calcification was present in 78% of subjects who had CT scans, and 60% of subjects who had lateral VFA scans. Ninety-seven of the 104 unevaluable scans were excluded due to overlying bowel gas and 7 were unevaluable due to obesity affecting the image quality. The mean total Agatston, total modified Agatston and total volume scores for VC measured using CT were 2442.6 ± 10129.9 AUs, 39787.4 ± 115565.8 AUs and 1.15 ± 4.57 cm3 respectively (Table 2). The mean total 24- and total 8-point scores for AAC as measured using lateral VFA images were 2.12 ± 2.42 and 1.19 ± 1.16 respectively (Table 2). Mean VC scores were calculated for each vascular site using CT. The AA and IA had the highest extent of calcification while the lowest incidence and extent of calcification was observed in the CA (Table 2). Univariate analysis revealed significant positive associations between measures of AAC on lateral VFA scans with measures of AAC on CT scans (Table 3), with the strength of association broadly equivalent between measures of AAC assessed on lateral VFA with AAC assessed on CT scans with r-values averaging 0.28.
Table 2 Calcium scores for individual vascular sites and total scores obtained using CT and lateral VFA.
| Scoring method |
Mean (SD) |
Range |
| CT Agatston (AU) |
|
|
| Total |
2442.6 (10129.9) |
0-98782 |
| Carotid arteries |
18.3 (108.0) |
0-1026 |
| Thoracic aorta |
202.19 (952.2) |
0-9355 |
| Abdominal aorta |
1294.9 (5548.6) |
0-55618 |
| Iliac arteries |
927.2 (3910.2) |
0-33733 |
| CT Modified Agatston (AU) |
|
|
| Total |
39787.4 (115565.8) |
0 - 1019091.2 |
| Carotid arteries |
447.1 (3000.0) |
0 - 29291.9 |
| Thoracic aorta |
3047.9 (11346.7) |
0 - 99876.5 |
| Abdominal aorta |
20727.2 (62411.7) |
0 - 551780.7 |
| Iliac arteries |
15565.1 (50491.4) |
0 - 366927.8 |
| CT Volume score (cm3) |
|
|
| Total |
1.151 (4.573) |
0 - 44.323 |
| Carotid arteries |
0.220 (0.990) |
0 - 0.490 |
| Thoracic aorta |
0.776 (1.895) |
0 - 4.260 |
| Abdominal aorta |
1.752 (3.397) |
0 - 24.860 |
| Iliac arteries |
1.736 (2.930) |
0 - 15.155 |
| VFA 24-point score |
|
|
| Total |
2.12 (2.42) |
0 - 11 |
| VFA 8-point score |
|
|
| Total |
1.19 (1.16) |
0 – 6 |
| AU; Arbitrary Units |
|
|
Table 3 Correlations between lateral VFA and CT VFA-matched* AAC scores.
| |
r |
p |
| 24-point score |
|
|
| Agatston |
0.29 |
0.006 |
| Modified Agatston |
0.29 |
0.005 |
| Volume |
0.29 |
0.006 |
| 8-point score |
|
|
| Agatston |
0.27 |
0.011 |
| Modified Agatston |
0.27 |
0.009 |
| Volume |
0.27 |
0.01 |
Table 4 shows the sensitivity, specificity, PPV, NPV and AUC of lateral VFA for detecting AAC measured using CT as the goldstandard. The presence of AAC was correctly identified in 33 (36%) subjects, with false negatives in 27 (30%) subjects who did have AAC (sensitivity 55%). Fifteen subjects were correctly identified as having no AAC with false positives identified in 16 subjects who did not have AAC (specificity 48%). The probability of subjects identified as having AAC as detected by lateral VFA scans that had AAC as measured by CT (PPV) was 67%, and the probability of subjects identified as having no AAC that were negative for AAC on CT (NPV) was 36%. The AUC was 0.52 for AAC. To investigate whether the accuracy of lateral VFA changed with different degrees of AAC as detected by CT, the sensitivity, specificity, PPV, NPV and AUC were calculated for tertiles of calcification (Table 4). Thresholds were set at each tertile of the variable for CT AAC scores resulting in the same values for sensitivity, specificity, PPV, NPV and AUC for each of the CT scoring methods. The measures with lateral VFA improved with increasing severity of AAC with moderately-good sensitivity: (64%, 83%), specificity: (55%, 56%) and AUC: (60% and 69%). Positive predictive values decreased from 67% to 39% while NPV increased from 36% to 90% with increasing severity of AAC. Receiver operating characteristic (ROC) for lateral VFA detecting AAC as measured by CT for the lowest to highest tertiles of AAC are shown in Figure 1. The sensitivity and AUC increased with each tertile 8 of AAC. The AUC at tertile 2 was found to be statistically significant from the AUC at tertile 1 and the binary cut-off (p=0.001).
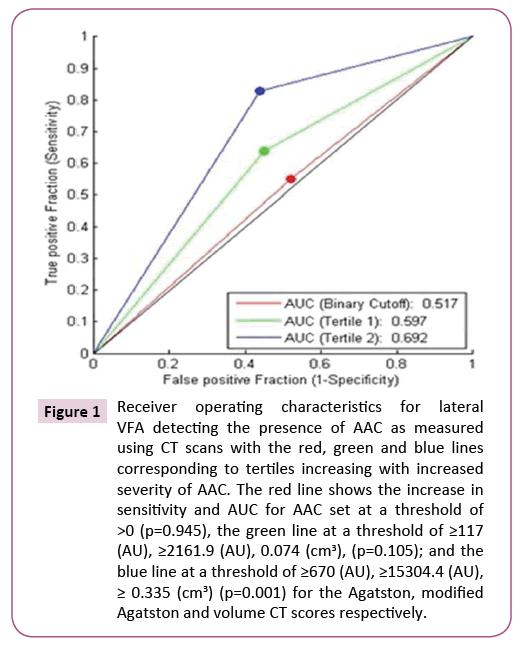
Figure 1: Receiver operating characteristics for lateral VFA detecting the presence of AAC as measured using CT scans with the red, green and blue lines corresponding to tertiles increasing with increased severity of AAC. The red line shows the increase in sensitivity and AUC for AAC set at a threshold of >0 (p=0.945), the green line at a threshold of ≥117(AU), ≥2161.9 (AU), 0.074 (cm3), (p=0.105); and the blue line at a threshold of ≥670 (AU), ≥15304.4 (AU), ≥ 0.335 (cm3) (p=0.001) for the Agatston, modified Agatston and volume CT scores respectively.
Table 4 The sensitivity, specificity, NPV, PPV and AUC associated with lateral VFA predicting AAC as detected by CT.
| CT AAC Score tertiles |
Sensitivity % |
Specificity % |
PPV % |
NPV % |
AUC (95%CI) |
| Binary cut-off >0 |
55 |
48 |
67 |
36 |
0.52 (0.38-0.62) |
| Tertile 1 |
64 |
55 |
55 |
64 |
0.60 (0.47-0.70) |
| Tertile 2 |
83 |
56 |
39 |
90 |
0.69 (0.55-0.80 |
*Abdominal aortic calcification as measured using CT was categorised as a binary cut-off point of0 for no calcium and 1 for calcium present, tertile 1 was categorised as scores ≥117AU for Agatston,≥2161.9AU for modified Agatston and ≥0.074cm3 for volume scores respectively and tertile 2 asscores ≥670 AU for Agatston, ≥15304.4AU for modified Agatston and ≥0.335cm3 for volumescores respectively
Relationship between vascular stiffness (PWV) and vascular calcification
Three hundred and sixty-two subjects (82%) from the total 444 subjects had carotid to femoral PWV performed with a mean PWV result of 8.8 ± 1.7. The distribution of scores was positively skewed (p ≤ 0.001) with a large proportion of subjects with a low PWV score. There were no significant correlations observed between PWV and AAC measured using lateral VFA in univariate analysis. In contrast, significant positive correlations were obtained when PWV was compared to VC measured using CT (Table 5). There were no independent associations between PWV and VC measured using the CT Agatston, modified Agatston and volume scores following adjustment for confounders associated with both arterial stiffness and VC including age, BMI, MAP and hypertension medication and smoking status (Table 6). Pearson’s correlations showed the three CT calcium scores to be highly correlated and were therefore included separately into the regression model to avoid collinearity. Age, BMI, MAP and the use of hypertension medication were all found to be significantly positively correlated with PWV, with age being the largest contributor to the regression model.
Table 5 Correlation between PWV and VC measured using CT.
| CT VC scoring method |
r |
p |
| Total Agatston |
0.39 |
<0.001 |
| Total modified Agatson |
0.4 |
<0.001 |
| Total volume |
0.39 |
<0.001 |
Table 6 Multi-linear regression analysis of arterial stiffness measured by PWV as the dependent variable and the total Agatston, total modified Agatston and total volume VC scores as independent variables.
| Variables |
R2 |
β-coefficients |
p-value |
| Agatston VC score (AU) |
0.4 |
0.051 |
0.0537 |
| Age (years) |
|
0.386 |
<0.001 |
| BMI (kg/m2) |
|
0.195 |
0.024 |
| MAP (mmHg) |
|
0.203 |
0.019 |
| Hypertension medication |
|
0.17 |
0.043 |
| Modified Agatston VC score (AU) |
0.393 |
-0.001 |
|
| Age (years) |
|
0.404 |
<0.001 |
| BMI (kg/m2) |
|
0.199 |
0.023 |
| MAP (mmHg) |
|
0.203 |
0.019 |
| Hypertension medication |
|
0.171 |
0.044 |
| Volume VC score (cm3) |
0.4 |
0.053 |
0.0528 |
| Age (years) |
|
0.386 |
<0.001 |
| BMI (kg/m2) |
|
0.195 |
0.024 |
| MAP (mmHg) |
|
0.203 |
0.019 |
| Hypertension medication |
|
0.17 |
0.043 |
Variables included in the model: Age, BMI, MAP, hypertension medication and smoking status.
Discussion
This study investigated the accuracy of lateral VFA for detecting AAC as measured using CT to determine whether lateral VFA scans could be utilised as a secondary utility to detect VC, in post-menopausal women referred for osteoporosis screening. CT is associated with increased radiation exposure and cost, and lateral VFA scans have been proposed as a reasonable substitute for detecting AAC which can be performed in minimal time with low radiation exposure and cost. Furthermore, the association was examined between PWV and VC measured using lateral VFA and CT scans to establish whether VC correlated with aortic stiffness, which is a strong independent predictor of CV mortality. The results show moderately-good sensitivity of lateral VFA for predicting AAC as measured by CT, and a significant positive association between PWV and VC as measured by CT.
Vascular calcification is an increasingly important clinical concern, particularly in populations with CKD, type 2 diabetes mellitus and atherosclerosis. The pathophysiology of VC is characterised by the deposition of calcium in the intima and/or media of the arterial wall, resulting in increased vascular stiffness. Most individuals aged 60 and over have calcification to some extent in their major arteries [30] leading to a reduction in arterial compliance which impairs CV haemodynamics, resulting in morbidity and possibly mortality [31-33]. Various diagnostic methods are currently used to assess VC, however there is an increased preference for simple, reliable, low radiation dose methods that can be readily implemented into routine clinical practice, such as lateral VFA scans for the semi-quantitative assessment of AAC, which can be performed concurrently with routine bone density screening. The use of lateral VFA for the assessment of AAC during screening for osteoporosis may be beneficial as a tool to identify asymptomatic patients at low to intermediate risk of a CV event, particularly the elderly, who may benefit from risk factor modification and further CV screening.
Although subjects included in the present study were healthy post-menopausal women with a lower risk of CVD, a large proportion of the cohort had VC, with 78% of subjects having VC detected by CT imaging and 60% having AAC as detected using lateral VFA imaging. The population in the present study had a mean age of 62 years which is a similar age to those reported as having increased AAC in other studies of low risk populations [34]; supporting the suggestion that AC is prevalent in later life and independent of known CV risk factors [6]. Subjects in the present study had a high extent of calcification within the AA and Iliac arteries (IA) which is similar to another recent study in a cohort of over 4500 subjects with a mean age of 56 years [30].
The present study reports moderate agreement between AAC measured using lateral VFA scans and VFA L1- L4 matched AAC scores measured using CT (Table 3). Although statistically significant, the correlations were weak accounting for less than 10% of the variance. The strength of association was broadly equivalent between the 24- and 8-point scores and each of the CT VFA-matched AAC scores. The correlations observed in the present study were lower than those reported by others [34]. However, the correlation between lateral VFA and CT is expected to be higher in subjects with greater amounts of calcification due to a larger range of values observed. Another important consideration is that there is a degree of inter-rater variability with the semiquantification of AAC from lateral VFA images. Furthermore, satisfactory scan data may not be available if 10 image quality is obscured by intestinal gas and/or obesity. Finally, it is impossible to state whether the moderate correlation seen between AAC measured using VFA and AAC measured using CT in the present study represents atherosclerotic burden or arteriosclerosis. Intimal or atherosclerotic calcification is characteristically patchy whereas arteriosclerotic or medial calcification is characteristically more diffuse in appearance but since the medial and intimal layers of the arterial lumen are in close proximity, it is not possible to distinguish between the two on either lateral VFA or CT images.
The present study reported moderately-good sensitivity with the lateral VFA 24-point score for predicting AAC as detected by the gold-standard of CT, which is consistent with results reported by others [34]. Moreover, the accuracy of lateral VFA imaging for predicting AAC on CT improved with the presence of a higher degree of AAC as detected on CT, which is also consistent with the results from studies on high risk CKD and dialysis patients [35]. Chronic kidney disease accelerates the development of atherosclerosis [36] and therefore a higher sensitivity reported with studies in patients with renal disease is likely to be a reflection of the greater extent of intimal calcification detected on lateral VFA scans in patients with CKD. The specificity of lateral VFA was lower than that reported by others, with studies reporting a higher specificity of 80% [34] and 75% [35]. Due to the subjective nature of calcium scoring on lateral VFA scan images, a proportion of scans were incorrectly identified as having calcification when calcium was not in fact present on CT (i.e., false positives). These results also reflect the subjectivity of calcium scoring on single-energy VFA scan images compared with dual-energy VFA scan images that are not disadvantaged by shadows and artefacts created by soft tissue. However, it is important to consider that the scan acquisition time for singleenergy VFA images is considerably quicker and with a lower radiation dose compared with dual-energy VFA, although some present-day scanners now operate with a reduced radiation exposure for dual-energy VFA. The AUC results from this study increased from 0.52 to 0.69 with increasing vascular burden on CT but only reached statistical significance at the highest tertile (Figure 1), and therefore indicate a moderate discriminatory value of lateral VFA in the presence of greater quantities of AAC. These ROC results are comparable to those reported elsewhere [34,35]. The negative and positive predictive values in the present study reflected the prevalence of AAC within this study population of lower risk post-menopausal women. In contrast, the NPV increased which was a reflection of the ability of lateral VFA to accurately predict when subjects did not have 11 AAC. Given the importance of PPV and NPV as a critical measure of the performance of lateral VFA for detecting AAC as measured on CT, the moderate scores obtained in the present study would not be adequate for detecting and quantifying low levels of AAC and demonstrate that lateral VFA may only provide an adequate substitute for CT for the detection of high levels of AAC in clinical practice, with values of 70% and higher considered acceptable. The NPV in the present study exceeded 70% only at the highest tertile where the greatest amounts of AAC were measured (Table 4). This perhaps should not be considered a negative finding since the use of lateral VFA to identify only those with more severe VC would seem a sensible approach to adopt in clinical practice due to the high incidence of AC with ageing. Reporting the results for only those with the greatest extent of calcification would limit referrals for further investigations to only those patients who may be at greatest risk of a CV event, and importantly avoid unnecessary concern to the patient.
Arterial stiffness as measured by PWV shows little or often no relation to conventional risk factors other than age and blood pressure [37]. Once considered to be largely dependent on atherosclerotic burden, arterial stiffness has been shown more recently to be related to calcified plaque and not non-calcified atheroma [38].
This study found no association between arterial stiffness measured using PWV and AAC as measured using lateral VFA scans (data not shown). These results were surprising considering the high incidence of AAC and increased arterial stiffness reported in this cohort of post-menopausal women, and that both PWV and VC increase with age with PWV primarily dependent on calcified plaque burden. Other research has reported a strong association between PWV and AAC measured using lumbar radiographs in both normal subjects from the general population and in chronic haemodialysis patients [38]. Therefore, the lack of association between PWV and AAC measured using lateral VFA in the present study may, once again, reflect the inter-rater variability of quantifying AAC on single-energy VFA scan images as already highlighted. Furthermore, because VFA imaging, like most imaging methods, is unable to distinguish between intimal and medial calcification, AAC quantified on lateral VFA images may reflect calcified atherosclerotic plaque burden in contrast to medial calcification which is more strongly associated with arterial stiffness.
Pulse wave velocity was initially found to be positively associated with VC as measured using CT. However, the positive associations with univariate analysis disappeared once adjusted for confounders in multivariate 12 analysis, including age, MAP and the use of anti-hypertensives which are significantly associated with arterial stiffness [39,40] which is consistent with findings reported by others [9].
This study had several limitations. It was limited to lower risk, post-menopausal women and results may not reflect those within the male population. Subjects who were known to be taking lipid lowering therapy were excluded, likely lowering both the incidence and extent of VC observed. Only 113 patients had CT scans of the chest and abdomen and the study used only moderate dose CT for image acquisition, unlike diagnostic CT scans used in clinical practice that require a higher radiation dose. The study did not compare single-energy acquired VFA images with those acquired using dual-energy, and the predictive value of PWV for detecting AAC was not assessed in this study.
Conclusion
This study reports moderately-good accuracy of lateral VFA scans for predicting high levels of AAC detected by CT. Results demonstrate that lateral VFA scans can provide a low radiation, low cost alternative to the ‘gold-standard’ of CT for evaluating AAC in a population of post-menopausal women referred for bone density screening for osteoporosis. This is the first study to assess the validity of lateral single-energy VFA scans for detecting AAC compared to CT with directly comparable regions of interest within the aorta. Further clinical studies are required to determine how well AAC measured by lateral VFA imaging correlates with aortic stiffness (PWV) particularly in older patients referred for bone densitometry measurements.
Funding Sources
This study was funded by the National Osteoporosis Society, a charity based in the UK.
References
- Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H,et al. (1998) Prediction ofcoronary heart disease using risk factor categories. Circulation 97: 1837-1847.
- Wilson PW, Kauppila LI, O'Donnell CJ, Kiel DP, Hannan M, et al. (2001) Abdominalaortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation 103: 1529-1534.
- Hollander M, Hak AE, Koudstaal PJ, Bots ML, Grobbee DE, et al. (2003) Comparison between measures of atherosclerosis and risk of stroke: the Rotterdam Study. Stroke 34:2367-2372.
- van der Meer IM, Bots ML, Hofman A, Iglesias del Sol A, van der Kuip DAM, et al. (2004) Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: theRotterdam Study. Circulation 109:1089-1094.
- Walsh CR, Cupples LA, Levy D, Kiel DP, Hannan M, et al. (2002) Abdominal aorticcalcific deposits are associated with increased risk for congestive heart failure: the Framingham Heart Study. Am Heart J 144:733-739.
- Toussaint ND, Lau KK, Strauss BJ, Polkinghorne KR, Kerr PJ (2010) Using vertebral bonedensitometry todetermine aortic calcification in patients with chronic kidney disease. Nephrology (Carlton) 15:575-583.
- Pencak P, Czerwieńska B, Ficek R, Wyskida K, Kujawa-Szewieczek A, et al. (2013) Calcification of coronary arteries and abdominal aorta in relation to traditional and novel risk factors of atherosclerosis in hemodialysis patients. BMC Nephrol 14:10.
- Suri P, Hunter DJ, Rainville J, Guermazi A, Katz JN (2012) Quantitative assessment of abdominal aorticcalcification and associations with lumbar intervertebral disc height loss: the Framingham Study. Spine J 12:315-323.
- Toussaint ND, Lau KK, Strauss BJ, Polkinghorne KR, Kerr PJ(2008) Associations between vascularcalcification, arterial stiffness and bone mineral density in chronic kidney disease. Nephrol Dial Transplant 23:586-593.
- Owen DRJ, Lindsay AC, Choudhury RP, Fayad ZA(2011) Imaging of atherosclerosis. Annu Rev Med62:25-40.
- Rumberger JA, Simons DB, Fitzpatrick LA, Sheedy PF, Schwartz RS (1994) Relation of coronary calciumdetermined by electron beam computed tomography and lumen narrowing determined by autopsy. Am J Cardiol 73:1169-1173.
- Kim KP, Einstein AJ, Berrington de Gonzalez A(2009) Coronary artery calcification screening: estimatedradiation dose and cancer risk. Arch Intern Med 169:1188-1194.
- Rea JA, Li J, Blake GM, Steiger P, Genant HK, et al. (2000) Visual assessment of vertebral deformityby X-ray absorptiometry: a highly predictive method to exclude vertebral deformity. OsteoporosInt11:660-668.
- Binkley N, Krueger D, Gangnon R, Genant H, Drezner M. (2005) Lateral vertebral assessment: a valuabletechnique to detect clinically significant vertebral fractures. OsteoporosInt 16:1513-1518.
- Vokes TJ, Dixon LB, Favus MJ(2003) Clinical utility of dual-energy vertebral assessment (DVA).OsteoporosInt 14:871-878.
- Schousboe JT, Wilson KE, Hangartner TN (2007) Detection of aortic calcification during vertebral fractureassessment (VFA) compared to digital radiography. PLoS One 2:e715.
- Schousboe JT, Debold CR(2006) Reliability and accuracy of vertebral fracture assessment withdensitometry compared to radiography in clinical practice. OsteoporosInt 17:281-289.
- Blacher J, Guerin AP, Pannier B, Marchais SJ, London GM(2001) Arterial calcifications, arterial stiffness,and cardiovascular risk in end-stage renal disease. Hypertension 38:938-942.
- Safar ME, Henry O, Meaume S(2002) Aortic pulse wave velocity: An independent marker of cardiovascular risk. Am J GeriatrCardiol 11:295-298.
- Blacher J, Asmar R, Djane S, London GM, Safar ME (1999) Aortic pulse wave velocity as a marker ofcardiovascular risk in hypertensive patients. Hypertension 33:1111-1117.
- Blacher J, Guerin AP, Pannier B, Marchais SJ, Safar ME, et al. (1999) Impact of aortic stiffness onsurvival in end-stage renal disease. Circulation 99:2434-2439.
- Pereira T, Maldonado J, Pereira L, Conde J (2013) Aortic stiffness is an independent predictor of stroke inhypertensive patients. Arq Bras Cardiol 100:437-443.
- Cruickshank K, Riste L, Anderson SG, Wright JS, Dunn G, et al. (2002) Aortic pulse-wave velocityand its relationship to mortality in diabetes and glucose intolerance: an integrated index of vascularfunction? Circulation 106:2085-2090.
- vanPopele NM, Grobbee DE, Bots ML, Asmar R, Topouchian J, et al. (2001) Association between arterial stiffness and atherosclerosis:The Rotterdam study. Stroke 32:454-460.
- Cecelja M, Jiang B, Bevan L, Frost ML, Spector TD, et al. (2011) Arterial stiffening relates toarterial calcification but not to noncalcified atheroma in women, a twin study. J Am Coll Cardiol 57:1480-1486.
- Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, et al. (1990) Quantification ofcoronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol 15:827-832.
- Broderick LS, Shemesh J, Wilensky RL, Eckert G, Zhou X-H, et al. (1996) Measurement of coronaryartery calcium with dual-slice helical CT compared with coronary angiography: Evaluation of CTscoring methods, interobserver variations, and reproducibility. AJR Am J Roentgenol 167:439-444.
- Callister TQ, Cooil B, Raya SP, Lippolis NJ, Russo DJ, et al. (1998) Coronary artery disease: improvedreproducibility of calcium scoring with an electron-beam CT volumetric method. Radiology 208:807-814.
- Asmar R, Benetos A, Topouchian J, Laurent P, Pannier B, et al. (1995) Assessmentof arterial distensibility by automatic pulse wave velocity measurement. Validation and clinical application studies. Hypertension 26:485-490.
- Allison MA, His S, Wassel CL, Morgan C, Ix JH, et al. (2012) Calcified atherosclerosisin different vascular beds and the risk of mortality. Arterioscler Thromb Vasc Biol 32:140-146.
- Keelan PC, Bielak LF, Ashai K, Jamjoum LS, Denktas AE, et al. (2001) Long-term prognostic value of coronary calcification detected by electron-beamcomputed tomography in patients undergoing coronary angiography. Circulation 104:412-417.
- Wayhs R, Zelinger A, Raggi P (2002) High coronary artery calcium scores pose an extremely elevated riskfor hard events. J Am Coll Cardiol 39:225-230.
- Arad Y, Spadaro LA, Goodman K, Newstein D, Guerci AD(2000) Prediction of coronary events withelectron beam computed tomography. J Am Coll Cardiol 36:1253-1260.
- Cecelja M, Frost ML, Spector TD, Chowienczyk P (2013) Abdominal aortic calcification detection usingdual-energy X-ray absorptiometry: validation study in healthy women compared to computedtomography. Calcif Tissue Int 92:495-500.
- Toussaint ND, Lau KK, Strauss BJ, Polkinghorne KR, Kerr PG (2009) Determination and validation of aorticcalcification measurement from lateral bone densitometry in dialysis patients. Clin J Am SocNephrol 4:119-127.
- Aikawa E, Aikawa M, Libby P, Figueiredo JL, Rusanescu G, et al. (2009) Arterial and aortic valve calcification abolished by elastolyticcathepsinS deficiency in chronic renal disease. Circulation 119:1785-1794.
- Cecelja M, Chowienczyk P (2009) Dissociation of aortic pulse wave velocity with risk factors forcardiovascular disease other than hypertension: A systematic review. Hypertension 54:1328-1336.
- Avramovski P, Janakievska P, Koneska M, Sotiroski K, Sikole A (2013) Associations between pulse wave velocity, aortic vascular calcification, and bone mineral density in chronic hemodialysis patients and general population. ISRN Vascular Medicine 2013: 507637.
- Cecelja M, Chowienczyk P (2012) Role of arterial stiffness in cardiovascular disease. JRSM Cardiovasc Dis 1:1-10.
- Avolio AP, Chen SG, Wang RP, Zhang CL, Li MF,et al. (1983) Effects of aging on changing arterial compliance and left ventricular load in a northern Chinese urban community. Circulation 68:50-58.