Keywords
Atorvastatin; Coronary slow flow; Choroidal
thickness; Spectral-domain optical coherence tomography;
Microcirculation abnormality
Introduction
The coronary slow flow (CSF) phenomenon is a frequent
angiographic clinical entity, characterized by delayed distal
vessel opacification in the absence of significant epicardial
coronary stenosis [1]. Previous histopathological studies have
shown the existence of the diffused hyperplastic fibromuscular
thickening of small arteries, as well as swelling and degeneration
of endothelial cells with narrowing of the vascular lumina in
most patients with CSF [2]. The early atherosclerosis, oxidative
stress, systemic inflammatory state, and the resultant
abnormalities in autacoids such as neuropeptide Y, endothelin-1,
and thromboxane A could be a pathogenetic mechanism of the
CSF [3,4]. Based on these data, it can be suggested that an
inappropriately high production of (and/or responsiveness to)
these vasoconstrictors might cause the increase in resting
microvascular resistance [5,6]. In addition, the CSF phenomenon
may be a component of systemic conditions that not only affects
the coronary arteries but also other arteries [7,8].
The choroid is a highly fenestrated, sinusoidal vascular plexus
and the site of the greatest blood flow in the body, comprising
up to 85% of the blood volume in the eye to nourish the outer
portion of retina. This vascular area has small arteries and veins
in outer segment and wider diameters of lumens in intermediate
layer and also capillary plexus in innermost layer [9]. It has been
shown that many pathogenic stimuli such as diabetes and
oxidative stress induce vascular dysfunction, leading to
atherosclerosis, ischemia, inflammation and thrombosis may
alter the regulation of retinal and choroidal blood flow [10].
According to recent studies, alteration in SFCT might be related
with microvascular dysregulation entities [11-14]. OCT is a
noninvasive and rapid method for multi-modal imaging the
retina and choroid. In combination with an enhanced depth
imaging (EDI) feature, SD-EDI OCT enables the identification of
specific layers within the retina in high resolution, as well as
deeper structures such as the choroid, in a way only previously
possible in histological samples [15].
Previous studies indicate that some of the cholesterolindependent
or “pleiotropic” effects of statins involve improving
endothelial function, enhancing the stability of atherosclerotic plaques, decreasing oxidative stress and inflammation, and
inhibiting the thrombogenic response [16]. Therefore, statins are
suggested in the treatment of CSF syndrome [17-19].
The aim of the present study is to evaluate the relationship
between CSF and SFCT. We also aimed to assess the possible
effect of short-term atorvastatin treatment on SFCT in patients
with CSF.
Methods
Study design and patient population
The study was designed to be an open-label study. Forty-six
patients with angiographically proven CSF but normal epicardial
coronary arteries and 43 healthy individuals were selected from
patients who had undergone diagnostic coronary arteriography
because of suspected coronary artery disease and were found to
have normal epicardial coronary arteries without CSF. All
patients and controls underwent baseline choroidal thickness
evaluation by using SD-OCT. After the ophtalmological
evaluation, atorvastatin 80 mg therapy was begun to all patients
with CSF. SFCT and serum lipid concentrations were performed
again after two weeks of follow-up.
Patients with a history of congestive heart failure, coronary
artery disease including spasm, plaque, or ectasia, valvular heart
disease, hyperthyroidism, chronic obstructive pulmonary
disease, ventricular preexcitation, atrioventricular conduction
abnormalities and those taking medications known to alter
cardiac conduction and retinochoroidal flow were excluded from
the study. Patients with a history of ocular disease (glaucoma,
arterial hypertension, uveitis, high myopia, age-related macular
degeneration, diabetes mellitus, etc.) and/or a history of
ophthalmic surgery that may have affected the choroidal
vascular network were also excluded. The study was approved
by local ethic committee according to the Declaration of Helsinki
and the patients gave written informed consent.
Ophtalmic examination and choroidal thickness
evaluation
All participants underwent a comprehensive examination
including visual acuity, intraocular pressure measurement, slitlamp
examination, dilated fundoscopy and SD-OCT. All SD-OCT
measurements were performed during the same daily interval
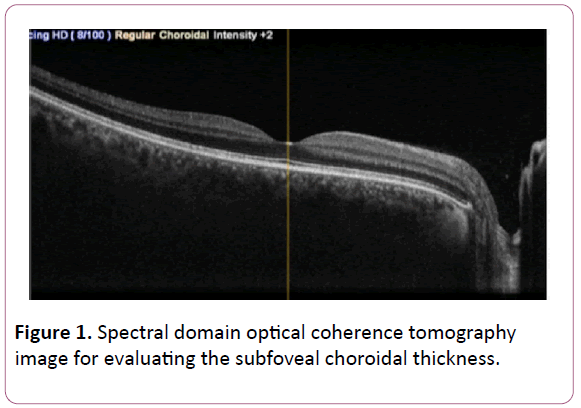
(10–12 am). The choroidal thickness was measured with SD-OCT
(RS-3000, Nidek) manually, on the horizontal EDI line scan, in 3
separate locations: subfoveal, and 2 mm nasal and 2 mm
temporal to the fovea. All choroidal thickness data were
assessed by the same ophthalmologist. Measurements were
performed in an area bounded by the outer limit of the retinal
pigment epithelium and the inner scleral border. Mean value of
both eyes were used for statistical analyzes(Figure 1). Choroidal
thickness measurements were repeated by one of the
ophthalmologist for a subset of images to calculate an intraobserver
correlation. Intra-observer variability was 0.92.
Figure 1: Spectral domain optical coherence tomography
image for evaluating the subfoveal choroidal thickness.
Coronary angiography and documentation of TIMI
frame count
Injection of contrast medium was carried out by an automatic
injector, at a speed of 3-4 mL/s for left coronary artery and 2-3
mL/s for right coronary arteriographies were recorded at a
speed of 25 frames/s. Coronary flow was quantified objectively
by an observers, who was blinded to the clinical details of the
individual participants. CSF was defined according to the
corrected TIMI frame count (TFC) method, and the subjects with
a TFC greater than 2 standard deviations (SD) from the published
normal range for the particular vessel were accepted as having
CSF.18
Statistical analysis
Statistical analysis was performed using the Statistical Package
for the Social Sciences (SPSS) for Windows (version 21.0; SPSS
Inc., Chicago, Illinois, USA). The assumptions for linearity and
homoscedasticity were tested based on the standardized
residuals plots, while the assumption of normality for the
dependent variable was tested using the Kolmogorov-Smirnov
criterion. Continuous variables are expressed as mean value ±
standard deviation (SD). Chi- square test was employed in order
to detect significant differences between categorical variables.
Differences between numeric variables of two groups were
tested with independent samples Student’s t-test for continuous
variables displaying normal distribution. Bivariate correlation
analyses were done by Pearson correlation test where
appropriate. The capacity of mean SFCT value in predicting
presence of CSF was analyzed using Receiver Operating
Characteristics (ROC) curve analysis. When a significant cut-off
value was observed, the sensitivity and specificity values were
presented. Statistical significance was accepted as p value less
than 0.05.
Results
Data of 48 patients with CSF (males=54.1%, age=51.49.3
years) and 41 healthy controls (males=48.8%, age=49.78.9 years)
were used in the analysis. CSF was observed in 3 vessels in 9
(18.7%) patients, in 2 vessels in 23 (47.9%) patients and in one
vessel in 16 (33.3%) patients. Left anterior descending artery (LAD) was affected in 38 (79.1%) patients, circumflex artery (Cx)
in 22 (45.8) patients and right coronary artery (RCA) in 29
(60.4%) patients.
The general, biochemical, choroidal characteristics, and TIMI
frame count for each major epicardial coronary artery of the
subjects are presented in Table 1. TIMI frame counts of controls
were significantly higher than patients with CSF compare. Mean,
left, and right SFCT of patients with CSF were significantly lower
than the measures of control group. There was no statistically
difference between patients and control group in both clinical
and biochemical data, except high sensitive C reactive protein
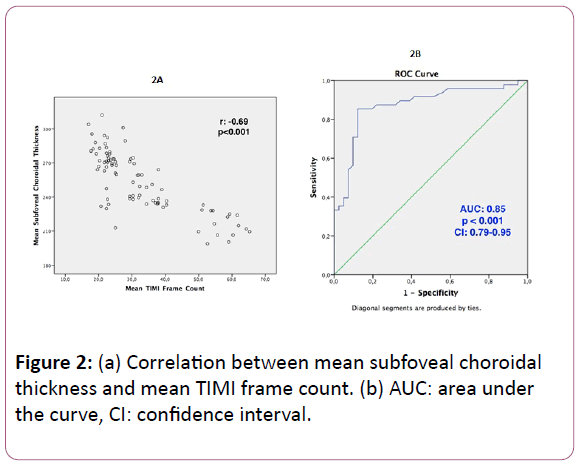
(hsCRP). There was significant negative correlation between
mean TIMI frame count and SFCT (r: -0.69, p<0.001) (Figure 2a).
ROC curve analysis revealed that a mean SFCT<259 μm
predicted CSF with 85% sensitivity and 88% specificity (area
under the curve: 0.85, p<0.001, confidence interval: 0.79-0.95)
(Figure 2b).
| |
Patients with CSF (n:48) |
Control group (n:41) |
p value |
| Clinical data |
| Age (years) |
51.4 ± 9.3 |
49.7 ± 8.9 |
0.37 |
| Male/female |
26/22 |
20/21 |
0.61 |
| BMI (kg/m2) |
26.7 ± 5.0 |
25.0 ± 3.1 |
0.09 |
| Systolic BP (mmHg) |
121.6 ± 7.9 |
122.7 ± 8.1 |
0.76 |
| Diastolic BP (mmHg) |
77.3 ± 4.2 |
78.1 ± 4.9 |
0.68 |
| Heart rate (bpm) |
74.3 ± 8.1 |
77.5 ± 8.9 |
0.89 |
| Smokers |
27 (56%) |
16 (39%) |
0.11 |
| TIMI frame count measurements |
| LAD* |
46.8 ± 15.8 |
21.8 ± 3.1 |
<0.001 |
| LCx |
40.3 ± 12.4 |
21.7 ± 3.1 |
<0.001 |
| RCA |
36.9 ± 10.7 |
22.1 ± 2.8 |
<0.001 |
| Mean TFC |
41.3 ± 12.1 |
21.9 ± 2.2 |
<0.001 |
| Subfoveal choroidal thickness measurements |
| Right subfoveal choroidal thickness (mm) |
236 ± 22 |
300 ± 18 |
<0.001 |
| Left subfoveal choroidal thickness (mm) |
240 ± 24 |
304 ± 19 |
<0.001 |
| Mean subfoveal choroidal thickness (mm) |
238 ± 23 |
302 ± 18 |
<0.001 |
| Biochemical data |
| Total cholesterol (mg/dl) |
200.3 ± 74.2 |
189.1 ± 70.1 |
0.39 |
| LDL- cholesterol (mg/dl) |
126.5 ± 63.1 |
118.3 ± 58.6 |
0.52 |
| HDL-cholesterol (mg/dl) |
43.8 ± 24.3 |
43.6 ± 24.2 |
0.78 |
| Triglyceride (mg/dl) |
136.7 ± 65.2 |
135.3 ± 64.7 |
0.64 |
| Hemoglobin (g/dl) |
13.4 ± 4.1 |
13.9 ± 3.2 |
0.32 |
| hsCRP (mg/L) |
3.9 ± 2.2 |
2.2 ± 1.5 |
0.02 |
Bold values indicate statistical significance p<0.05.
Abbreviations: BMI: body-mass index; BP: blood pressure; HDL: high-density lipoprotein; hsCRP: high-sensitivity C-reactive protein; RCA: right coronary artery; TFC: TIMI frame count; LAD=left anterior descending; LCx: left circumflex; LDL: Low-density lipoprotein
* Corrected TFC was given for the LAD artery.
Table 1: Demographic, angiographic, choroidal, and biochemical
characteristics of the patients.
Figure 2: (a) Correlation between mean subfoveal choroidal
thickness and mean TIMI frame count. (b) AUC: area under
the curve, CI: confidence interval.
SFCT measurements and biochemical characteristics before
and after atorvastatin therapy are presented in Table 2. Mean
SFCT increased from 238 ± 23μm to 262 ± 21 μm after 2 weeks
atorvastatin therapy (p<0.001), but it was still statistically
thinner than healthy controls (262 ± 21 μm vs. 302 ± 18 μm,
p<0.001). There were no statistically significant difference after
atorvastatin therapy in biochemical characteristics.
| |
Before therapy (n:48) |
Two weeks after atorvastatin therapy (n:48) |
Control group (n:41) |
p valueα |
p valueβ |
| Choroidal thickness measurements |
| Right choroidal thickness (mm) |
236 ± 22 |
261 ± 20 |
300 ± 18 |
<0.001 |
<0.001 |
| Left choroidal thickness (mm) |
240 ± 24 |
263 ± 21 |
304 ± 19 |
<0.001 |
<0.001 |
| Mean choroidal thickness (mm) |
238 ± 23 |
262 ± 21 |
302 ± 18 |
<0.001 |
<0.001 |
| Biochemical data |
| Total cholesterol (mg/dl) |
200.3 ± 74.2 |
192.4 ± 72.4 |
189.1 ± 70.1 |
0.45 |
0.73 |
| LDL-cholesterol (mg/dl) |
126.5 ± 63.1 |
123.5 ± 59.7 |
118.3 ± 58.6 |
0.59 |
0.55 |
| HDL-cholesterol (mg/dl) |
43.8 ± 24.3 |
44.6 ± 25.2 |
43.6 ± 24.2 |
0.12 |
0.09 |
| Triglyceride (mg/dl) |
136.7 ± 65.2 |
122.3 ± 59.8 |
135.3 ± 64.7 |
0.08 |
0.1 |
| Hemoglobin (g/dl) |
13.4 ± 4.1 |
13.8 ± 4.2 |
13.9 ± 3.4 |
0.24 |
0.48 |
| hsCRP (mg/L) |
3.9 ± 2.2 |
2.9 ± 1.8 |
2.2 ± 1.5 |
0.07 |
0.02 |
Bold values indicate statistical significance p<0.05.
Abbreviations: HDL: high-density lipoprotein; hsCRP: high-sensitivity C-reactive protein; LDL: Low-density lipoprotein.
α statistically difference between coronary slow flow patients before and after short-term atorvastatin therapy.
β statistically difference between coronary slow flow patients after short-term atorvastatin therapy and control group.
Table 2: Subfoveal Choroidal thickness measurements and biochemical characteristics of the patients before and after atorvastatin
therapy in patients with coronary slow flow and healthy subjects.
Discussion
In present study, we observed significantly lower SFCT in
patients with CSF compared with controls and there was a
significant negative correlation between mean TIMI frame count
and SFCT before short-term atorvastatin therapy. Short-term
atorvastatin therapy resulted in a significant increase in SFCT,
but it was still lower than healthy control group. To the best of
our knowledge our study is the first study that evaluates SFCT in
patients with CSF.
There have been many reports of coronary microcirculation
abnormality associated with early atherosclerosis and systemic inflammatory state leading to endothelial dysfunction and
increase of resting microvascular resistance in CSF phenomenon
[20,21]. The CSF phenomenon may not only affect the coronary
arteries but it may also be a part of vascular problem that affect
other arteries. Sezgin et al. reported the endothelial dysfunction
by using flow-mediated dilatation of the brachial artery in
patients with CSF [6].
Arteriosclerotic processes and vasoconstriction resulted from
oxidative stress entity and resultant increased autocoid levels,
might be susceptible to choroidal microcirculation abnormality.
It has been shown in animal models that arteriosclerotic
changes occur in retina and choroid [22]. Recent studies related
with microcirculation abnormality showed the thinning of SCFT
in patients with retinitis pigmentosa [11-13] and chronic kidney
disease [10] by using SD-OCT measurements. The seemingly
obvious connection between the vascular components of the
choroid and other vascular beds of the body has produced a
number of studies on the relationship between SFCT and various
cardiovascular diseases. Ahmad et al. [23] showed that patients
with coronary artery diseases had a thinner macular choroid
than controls and Altinkaynak et al. [24] showed that patients
with congestive heart failure presented lower SFCT compared to
age- and gender-matched controls. A single study evaluated the
relationship between hypercholesterolemia and SFCT, showing
SFCT to be significantly higher in patients with increased total
cholesterol compared to controls [25]. If there were reduction in
serum lipid profile, we would found decrease in SFCT values. In
our study, there were no statistically significant differences
between before and after serum lipid profile so increase of SCFT
after statin therapy might be a reflection of generalized microvascular improvement and pleiotropic affect of short-term
statin therapy.
Caliskan et al. explored the coronary flow reserve increase
with atorvastatin therapy due to its anti-inflammatory effect in
patients with CSF [26]. In addition, Cakmak et al. also
demonstrated that simvastatin improved myocardial perfusion
abnormality in patients with CSF [16]. Recently Ling et al. have
shown that statin therapy improved peripheral endothelial
dysfunction in CSF patients [17]. Hinoi et al. demonstrated the
potent vasorelaxing effect of atorvastatin treatment on coronary
microvessels in patients with normal epicardial coronary arteries
[27]. We could not perform control coronary angiography to our
patients with CSF after atorvastatin therapy. Hence, evaluation
of the direct effect of statin therapy on coronary flow is not
possible. However, increase in SFCT after statin therapy in these
patients might be a reflection of improvement of
microcirculation abnormality in choroidal plexus and possibly
generalized endothelial function.
Improvement in endothelial functions with statin therapy
might be related with anti-inflammatory effects of atorvastatin
in our study which was reflected by a decrease in hsCRP levels. Li
et al. showed that the plasma concentration of hsCRP increased
in CSF patients compared with control group [28].
Our study has important clinical implications. Effects of
medications for the treatment of patients with CSF may be
assessed by measuring SCFT in clinical practice. This is especially
relevant in patients without any indication for repeat coronary
angiography.
Study limitation
There are some important limitations of this study. The first
limitation of this study is small sample size. Second, local ethic
committee did not approve to perform control coronary
angiography after statin treatment. If we had been able to
perform control angiography, this would have added much more
significant data to our study. Third, comparison of affect of other
statins on SFCT in patients with CSF might reinforce our
hypothesis. Moreover, the evaluation of short- and long-term
affect of statin therapy with larger study population may
improve clinical implication of our study.
Conclusion
Present study demonstrated for the first time the relationship
between CSF phenomenon and SFCT by using SD-OCT.
Microvascular dysregulation might be operative in both
coronary and choriocapillary arteries as a systemic disorder in
patients with CSF. Short-term atorvastatin theraphy was
effective in the increase of SFCT, which may be an index of
improvement of microvascular abnormality in patients with CSF.
Author Contributions
Dr. Batur Kanar was the primary investigator of the study. He
was responsible for the design of the study, data collection,
analysis of the data and drafting of the article. Dr. Hatice Selen
Kanar was responsible for data collection and analysis of the
data.
References
- Mangieri EMG, Ciavolella M (1996) Slow coronary flow: clinical and histopathological features in patients with otherwise normal epicardial coronary arteries. Cathet Cardiovasc Diagn37: 375-381.
- Beltrame JF, Limaye SB, Wuttke RD, Horowitz JD (2003) Coronary hemodynamic and metabolic studies of the coronary slow flow phenomenon. Am Heart J 146: 84-90.
- Beltrame JF, Limaye SB, Horowitz JD (2002) The coronary slow flow phenomenon--a new coronary microvascular disorder. Cardiology 97: 197-202.
- Karatzis EN (2005) The role of inflammatory agents in endothelial function and their contribution to atherosclerosis. Hellenic J Cardiol 46: 232-239.
- Wang X, Nie SP (2011) The coronary slow flow phenomenon: characteristics, mechanisms and implications. Cardiovasc Diagn Ther 1: 37-43.
- Camsari A, Pekdemir H, Ciçek D, Katircibasi T, Parmaksiz T, et al. (2004) Endothelin-1 and nitric oxide levels in patients with mitral annulus calcification. Jpn Heart J 45: 487-495.
- Sezgin AT, Sigirci A, Barutcu I, Topal E, Sezgin N, et al. (2003) Vascular endothelial function in patients with slow coronary flow. Coron Artery Dis 14: 155-161.
- Wang X, Geng LL, Nie SP (2010) Coronary slow flow phenomenon: a local or systemic disease? Med Hypotheses 75: 334-337.
- Liu CH, Wang Z, Sun Y, Chen J (2017) Animal models of ocular angiogenesis: from development to pathologies. FASEB J 31: 4665-4681.
- Hirase T, Node K (2012) Endothelial dysfunction as a cellular mechanism for vascular failure. Am J Physiol Heart Circ Physiol 302: 499-505.
- Balmforth C, van Bragt JJ, Ruijs T, Cameron JR, Kimmitt R, et al. (2016) Chorioretinal thinning in chronic kidney disease links to inflammation and endothelial dysfunction. JCI Insight 1: 1-13.
- Finzi A, Cellini M, Strobbe E, Campos EC (2014) ET-1 plasma levels, choroidal thickness and multifocal electroretinogram in retinitis pigmentosa. Life Sci 118: 386-390.
- Kim H, Lee SC, Kwon KY, Lee CS (2016) Subfoveal choroidal thickness as a predictor of treatment response to anti-vascular endothelial growth factor therapy for polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol 254: 1497-1503.
- Sorrentino FS, Bonifazzi C, Perri P (2015) The Role of the Endothelin System in the Vascular Dysregulation Involved in Retinitis Pigmentosa. J Ophthalmol 2015: 1-6.
- Leitgeb RA, Werkmeister RM, Blatter C, Schmetterer L (2014) Doppler optical coherence tomography. Prog Retin Eye Res 41: 26-43.
- Liao JK, Laufs U (2005) Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol 45: 89-118.
- Cakmak M, Tanriverdi H, Cakmak N, Evrengul H (2008) Simvastatin may improve myocardial perfusion abnormality in slow coronary flow. Cardiology 110: 39-44.
- Ling MC, Ruddy TD, de Kemp RA, Ukkonen H, Duchesne L (2005) Early effects of statin therapy on endothelial function and microvascular reactivity in patients with coronary artery disease. Am Heart J 149: 1137.
- Gibson CM, Cannon CP, Daley WL Dodge JT Jr, Alexander B Jr, et al. (1996) TIMI frame count: a quantitative method of assessing coronary artery flow. Circulation 93: 879-888.
- Gori T, Fineschi M (2012) Two coronary "orphan" diseases in search of clinical consideration: coronary syndromes x and y. Cardiovasc Ther 30: 58-65.
- Fineschi M, Bravi A, Gori T (2008) The "slow coronary flow" phenomenon: evidence of preserved coronary flow reserve despite increased resting microvascular resistances. Int J Cardiol 127: 358-361.
- Salazar JJ, Ramírez AI, de Hoz R, Rojas B, Ruiz E, et al. Alterations in the choroid in hypercholesterolemic rabbits: reversibility after normalization of cholesterol levels. Exp Eye Res 8: 412-422.
- Ahmad M, Kaszubski PA, Cobbs L, Reynolds H2, Smith RT (2017) Choroidal thickness in patients with coronary artery disease. PLoS One 12: 1-12.
- Altinkaynak H, Kara N, Sayın N, Güneş H, Avşar S, et al. (2014) Subfoveal choroidal thickness in patients with chronic heart failure analyzed by spectral-domain optical coherence tomography. Curr Eye Res 39: 1123-1128.
- Wong IY, Wong RL, Zhao P, Lai WW (2013) Choroidal thickness in relation to hypercholesterolemia on enhanced depth imaging optical coherence tomography. Retina 33: 423-428.
- Caliskan M, Erdogan D, Gullu H, Topcu S, Ciftci O, et al. (2007) Effects of atorvastatin on coronary flow reserve in patients with slow coronary flow. Clin Cardiol 30: 475-479.
- Hinoi T, Matsuo S, Tadehara F, Tsujiyama S, Yamakido M (2005) Acute effect of atorvastatin on coronary circulation measured by transthoracic Doppler echocardiography in patients without coronary artery disease by angiography. Am J Cardiol 96: 89-91.
- Li JJ, Qin XW, Li ZC, Zeng HS, Gao Z. et al. (2007) Increased plasma C-reactive protein and interleukin-6 concentrations in patients with slow coronary flow. Clin Chim Acta 385: 43-47.