Enrique Chacon-Cruz1*, Jorge Arturo Alvelais-Palacios2, Erika Zoe Lopatynsky-Reyes 2 Jaime Alfonso Rodriguez-Valencia3 and Maria Luisa Volker-Soberanes4
1Department of Pediatric Infectious Diseases, Hospital General de Tijuana, Tijuana, Baja-California, Mexico
2School of Medicine, ECISALUD-Campus Universidad Autonoma de Baja California, Mexico
3Department of Pediatrics, Hospital General de Tijuana, Tijuana, Baja-California, Mexico
4Department of Microbiology, Hospital General de Tijuana, Tijuana, Baja-California, Mexico
Corresponding Author:
Chacon-Cruz E
Department of Pediatric Infectious Diseases
Hospital General de Tijuana, Baja-California
Mexico
Tel: +52-664-6346820
E-mail: echacon88@hotmail.com
Received date: March 28, 2017; Accepted date: April 06, 2017; Published date: April 16, 2017
Citation: 2017 Enrique Chacon-Cruz. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Copyright: © Chacon-Cruz E, Alvelais-Palacios JA, Lopatynsky-Reyes EZ, Rodriguez-Valencia JA, Volker-Soberanes ML. Meningococcal Disease in Children: Eleven Years of Active Surveillance in a Mexican Hospital and the Need for Vaccination in the Tijuana Region. J Infec Dis Treat 2017, 3:1.
Keywords
Meningococcal disease; Active surveillance; Bacterial meningitis; Children; Mexico
Introduction
In Mexico, Meningococcal Disease (MD) is considered to be a rare condition, with total number of cases in the whole country as low as 2 cases per year, with rates much lower (reaching as low as 0.06/100, 000 population) [1] than prevaccination rates reported in the US (0.53/100, 000) [2] Argentina (0.7/100, 000) [3] and Brazil (1.9/100, 000) [3]. Low rates of MD in Mexico are based on passive surveillance and under reporting we think is a major concern. Accordingly, we have already published a 3 years binational study comparing MD incidence on the Tijuana, Mexico and San Diego, California border (the highest transited frontier in the world). Our publication revealed that in Tijuana, MD was not lower than in San Diego [4]. This was the first study that actually showed that MD is significantly present in Mexican territory.
Furthermore, from January 30th March/30th 2013, we dealt with an outbreak of MD, with 19 culture-confirmed cases and 7 deaths [5] and also published a National active surveillance study in nine Hospitals throughout the country, proving that MD is present in the north part of Mexico [6]. However, Health Authorities still hesitate to vaccinate against MD in the region.
The main purpose of this paper is to improve the amount of clinical and epidemiological information for MD based on eleven years of active (prospective) surveillance only in our hospital, but also this study, along with others mentioned above, will help to convince Health Authorities to seriously consider vaccination in this geographic area.
Materials and Methods
Since October-2005 until September-2016 (eleven years), active surveillance looking for all patients admitted with suspected MD< 16 years of age was performed at the Tijuana, Mexico, General Hospital (TGH). Active surveillance as definition is “syndromatic” and prospective and it was performed as follows: All patients < 16 years of age with clinical signs and symptoms of acute meningitis, clinical febrile purpura and/or sepsis were included to confirm or rule out MD. Once the patient was admitted, both blood and CSF samples were taken for cytological and chemical testing, as well as immediately put into enriched broth-media and followed by rapid (less than 3 minutes) incubation at 37°C with 5% of CO2.
Confirmation of MD was done by conventional isolation from all positive broth media cultures. For all Neisseria meningitidis isolates, serogroup identification was performed by the Pastorex meningitis kit (Alere, Ltd®, Stockport, UK).
Among survivors, all were discharged with a brain`s CT scan and consulted three months later to search for any neurological, audiological and other type of sequelae (these evaluations were done by the Departments of Infectious Diseases, Otorhinolaryngology and Neurology).
Descriptive data was analyzed using Excel®. Comparative analysis was performed using VassarStat®, both chi-square and z-tests were used when needed.
Hospital’s standard of care was implemented for every patient admitted and patient’s (parent or tutor) consent form was the same that is used in the hospital. Datasheet containing information of every patient did not show names or other forms to expose patient’s identity, this datasheet is only kept with the corresponding author of this study and only privately showed when the hospital’s IRB requires information. The hospital’s IRB accepted the study based on these specifications.
PCR and/or other molecular biology methods for bacterial and/or viral identification were not used due to the lack of economic support.
To estimate MD attack rates, first is relevant to have a perspective of the Mexican-National Health System, which is divided into four “Health Insurances”: “IMSS” (Mexican Insurance for Social Workers), “ISSSTE” (Insurance for Federal- Goverment Workers), “ISSSTE-per State” (Insurance for State- Goverment Workers) and “Seguro Popular” (“Popular Insurance”) which is related to the rest of the population not covered to all others Insurance systems. Our Hospital belongs to “Seguro Popular” and all patients in that Health-Insurance system who live in Tijuana only attend the TGH when needed, accordingly, our denominators to estimate MD attack rates, were the population by age who belong to “Seguro Popular”.
Results
There were 51 MD cases. Median age was of 36 months (3 days-15 years), with 21 (41.18%) < 2 years old. Twenty eight (55%) were male and 23 (45%) female. With the exception of three patients (5.88%) who had a predisposing condition (Lupus, HIV infection and Leukemia), all others had no clinical records of any hospitalization in the past.
Twenty patients (39.2%) had an upper respiratory tract infection before MD developed and 18 (35.3%) received oral antibiotics prior to admission (55.55% received amoxicillin with/without clavulanic acid). All but two patients were born in Tijuana, all patients > 1 year old have lived in Tijuana for at least six months. Only one patient had the tetravalent (A, C, Y, W) meningococcal conjugate vaccine, but this child developed a serogroup B related MD. Median days of illness prior to admission was of two (1-14). At admission, 47 (92.15%) had meningitis, 24 (47%) purpura, 4 (7.84%) conjunctivitis and 2 (3.92%) pleural effusion (both patients with pleural effusion had a serogroup Y related MD).
Yearly cases are shown in Figure 1 with an average yearly number of cases of 4.63. It is relevant to mention that six of the eight patients in the 2012-2013 periods were part of an outbreak during 2013 [5].
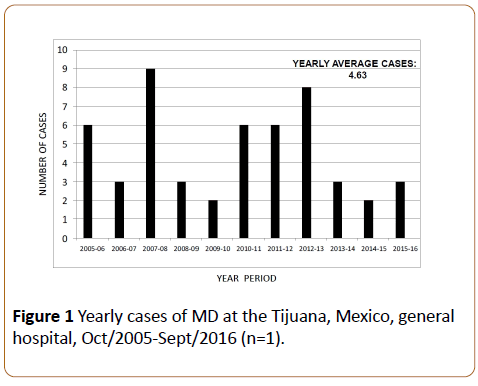
Figure 1: Yearly cases of MD at the Tijuana, Mexico, general hospital, Oct/2005-Sept/2016 (n=1).
Serogroup distribution was as follows: C-32 (62.74%), Y-12 (23.53%), B-5 (9.8%) and Ignored-2 (3.92%). Median hospitalization days were of 10 (1 hour-44 days). Overall fatality was of 13 (25.49%). At admission, presence of thrombocytopenia, leukopenia and purpura were significantly associated with mortality (p< 0.05). Among survivors (n=38), 13 (34.2%) developed sequelae, including cortical atrophia (confirmed by the CT scan), hearing and/or motor disabilities and skin scars. In the same time period, there were 103 patients admitted with potentially bacterial meningitis (acute meningitis with white blood cells > 10/mm3 and at least 50% by polymorphonuclear leukocytes in the CSF), from which 80 (77.67%) had positive cultures. As shown in Figure 2, N. meningitidis was responsible for 47 (58.75%) of all cultureconfirmed bacterial meningitis, followed by S. pneumoniae (18=22.5%) and others.
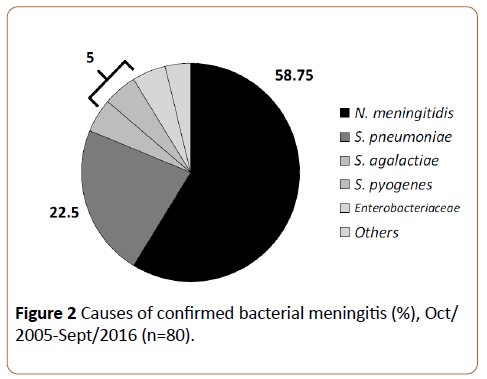
Figure 2: Causes of confirmed bacterial meningitis (%), Oct/ 2005-Sept/2016 (n=80).
Based on the population covered by TGH (so called “Seguro Popular or Popular Insurance”, mentioned above in the Methods section), as shown in Figure 3, yearly average MD attack rates were of 7.61 and 2.69 per 100,000 population in children < 2 and < 16 years of age, respectively.
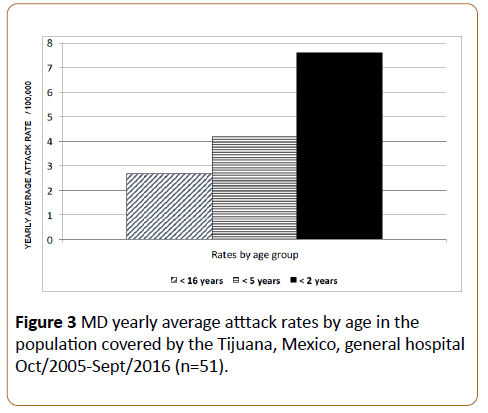
Figure 3: MD yearly average atttack rates by age in the population covered by the Tijuana, Mexico, general hospital Oct/2005-Sept/2016 (n=51).
Discussion
This study confirms that MD is endemic in Tijuana. TGH is the only hospital en the region with active surveillance and trained microbiologists to identify and serogroup N. meningitidis, being the main reason why is the only hospital with reliable data regarding the real incidence of this disease.
Our study, following eleven years of active surveillance, not only confirms that MD is endemic in this Northwest part of Mexico (contrary to what has been published by National Reports) [1] but also gives significant clinical, epidemiological and microbiological information of the disease. It is the longest active surveillance for MD in Mexico and may be among the longest in Latin America [3,7].
Furthermore, the information obtained during these eleven years gives significant information of MD in the region including the following:
First of all, proves that N. meningitidis is the leading cause of bacterial meningitis (58.75%).
Secondly, lethality is high (25.5%) and among survivors sequeleae was detected in one third of patients.
Third, shows that MD in the region behaves as an endemic disease, affecting mostly young infants and the presence of an outbreak by MD serogroup C (CT-11) occurred [5].
Fourth, at least 86% of cases were caused by serogroups included by the tetravalent (A,C,Y, W) conjugate meningococcal vaccine.
In Latin America, the first country that implemented meningococcal vaccination against MD is Brazil, which started in the year 2010 using the monovalent - C meningococcal conjugated vaccine, a decision based on their epidemiology, with an overall estimated rate of 1.9/100, 000 population and higher prevalence of serogroup C [3,8]. Other Latin American countries show different serogroup distribution, such as prevalence of serogroup B and emergence of W in Argentina and Chile [3,9-11]. Furthermore, in Chile, an outbreak by MD serogroup W (ST-11) occurred in 2013 [10,11] and vaccine implementation was promptly implemented [12].
Monovalent -C meningococcal conjugated vaccine was introduced in the United Kingdom over a decade ago, with a significant decrease of MD by serogroup-C and very little increase by other serogroups (especially serogroup Y). In the US, the implementation of tetravalent conjugated meningococcal vaccine in 2005 has decreased serogroupsvaccine included MD cases [13-16].
For Mexico, MD is considered a disease of immediate notification, nevertheless, all of the latter is based on passive surveillance and National reports show very low rates for MD in the country [1]. We do believe that underreporting due to unawareness of MD is the main reason for this problem, but may be other reasons could explain this (underreporting directly from medical doctors and hospitals, among others).
Based on our findings in Tijuana, Mexico, we performed a National Mexican Network based on active surveillance for meningitis in children from nine hospitals: This study proved that by using active surveillance, MD was present mostly in the north part of the country, with 75% of cases in Tijuana [6].
Analysis for both environmental issues with clinical presentations, as well as studies looking for nasopharyngeal colonization both in children and adults should be consider in the future to look for potential reason of the higher endemicity of MD in the Tijuana region.
It is relevant to mention that at least in Mexico, active surveillance is indeed a much more useful tool to more accurately determine incidence of MD than passive surveillance and currently active surveillance is preferred internationally as a much better tool to identify and describe MD [17-19]. Active surveillance not only identify cases, but also provides significantly higher information such as hospitalization length, complications, sequelae, among many others issues and future studies looking at vaccine’s costeffectiveness can be better performed from data obtained from studies done by active surveillance [17-19].
Regardless of the lack of cost-effectiveness studies developed in the Tijuana region, only based on WHO recommendations, vaccination in our city should be seriously evaluated by Health Authorities [20].
Conclusions
After eleven years of active surveillance, MD is endemic in Tijuana, Mexico.
Lethality is high and affects mostly young infants, with an outbreak in adolescents and young adults in 2013.
Based on all of the above, meningococcal vaccination should be seriously considered in the region [20].
References
- Almeida GL, Franco PC, Perez LF, Santos PJL (2004) Enfermedadpormeningococo, Neisseria meningitidis: perspectivaepidemiológica, clínica y preventiva. Sal Pub Mex 46: 438-450.
- Chang Q, Tzeng YL, Stephens DS (2012) Meningococcal disease: changes in epidemiology and prevention. ClinEpidemiol 4: 237-245.
- Safadi MAP, Cintra OAL (2010) Epidemiology of meningococcal disease in Latin America: current situation and opportunities for prevention. Neurol Res 32: 263-271.
- Chacon CE, Sugerman DE, Ginsberg MM, Hopkins J, Hurtado M JA, et al. (2011) Surveillance for invasive meningococcal disease in children, US-Mexico border, 2005- 2008. Emerg Infect Dis 17: 543-546.
- Chacon CE, Espinosa DL, Monteros LE, Navarro AS, Aranda LJL, et al (2014) An outbreak of serogroup C (ST-11) meningococcal disease, in Tijuana, Mexico. TherAdvVacc 2: 71-76.
- Chacon CE, Martinez LCA, Llausas ME, Luevanos VA, Vazquez NJA et al. (2016) Neisseria meningitidis and Streptococcus pneumoniae as leading causes of pediatric bacterial meningitis in nine Mexican hospitals following 3 years of active surveillance. TherAdvVacc 4: 15-19.
- Brayer AF, Humiston SG (2011) Invasive meningococcal disease in childhood. Pediatr Rev 32: 152-161.
- Pan American Health Organization (2013) Informe regional de SIREVA II, Datosporpaís y porgrupos de edadsobrelascaracterísticas de los aislamientos de Streptococcus pneumoniae, Haemophilusinfluenzae y Neisseria meningitidis, en procesosinvasivosbacterianos. Available from: https://iris.paho.org/xmlui/handle/123456789/31147
- Ibarz PAB, Lemos AP, Gorla MC, Regueira M (2012) Sireva Working Group II laboratory-based surveillance of Neisseria meningitidis isolates from disease cases in Latin American and Caribbean countries, Sireva II 2006-2010. PLoS One 7: e44102.
- Matute I, Olea A, Lopez D, Loayza S, Najera M, et al. (2015) Clinical features and prognostic factors of meningococcal disease: a case series study in Chiile during the 2012-2013 outbreaks. Rev ChlienaInfectol 32: 505-516.
- Lopez EL, Debbag R (2012) Meningococcal disease: always present. Serogroup changes in the Southern Cone. Rev ChilenaInfectol 29: 587-594.
- Chile begins campaign of vaccination against meningitis by unusual outbreak (2012)
- Ladhani SN, Flood JS, Ramsay ME (2012) Invasive meningococcal disease in England and Wales: implications for the introduction of new vaccines. Vaccine 30: 3710.
- Agrawal S, Nadel S (2001) Acute bacterial meningitis in infants and children: epidemiology and management. Paediatr Drugs 13: 385-400.
- Cohn AC, MacNeil JR, Harrison LH (2010) Changes in Neisseria meningitidis disease epidemiology in the United States, 1998-2007: implications for prevention of meningococcal disease. Clin Infect Dis 50: 184-191.
- Baccarini C, Ternouth A, Wieffer H (2012) The changing epidemiology of meningococcal disease in North America 1945-2010. Hum VaccinImmunother 9: 162- 171.
- Safadi MA, O`Ryan M, Valenzuela BMT, Brandileone MC, Gorla MC, et al. (2015) The current situation of meningococcal disease in Latin America and updated Global Meningococcal Initiative (GMI) recommendations. Vaccine 27: 6529-6536.
- Gentile A, Bakir J, Agosti MR, Ensinck G, Abate H, et al. (2016) Meningococcal disease in children in Argentina: A three-year active sentinel hospital surveillance study. Pediatr Infect Dis Jpp: 28.
- Ahmed SS, Oviedo OE, Mekary SR, Freifeld CC, Tougas G, et al. (2015) Surveillance for Neisseira meningitides disease activity and transmission using information technology. PLOS One pp: 20.
- WHO Position Paper (2011) Meningococcal Vaccines: Weekly epidemiological record, Available from: https://www.ncbi.nlm.nih.gov/pubmed/22128384.