Adel El-Badrawy1*, Basma Gadelhak1, Mohammad K El-Badrawy2, Shahira Ali El-Etreby3, Ziad Emarah4 and Hatem Elalfy5
1Department of Radiology, Mansoura University, Egypt
2Department of Chest Medicine, Mansoura University, Egypt
3Department of Internal Medicine, Mansoura University, Egypt
4Department of Medical Oncology, Oncology Center, Mansoura University, Egypt
5Department of Endemic Medicine, Mansoura University, Egypt
*Corresponding Author:
Adel El-Badrawy
Professor, Faculty of Medicine
Department of Radiology
Mansoura University, Egypt
Tel: +002-0100-5785751, 002-050-2234683
Fax: 002-050-2315280
E-mail: adelelbadrawy@hotmail.com
Received Date: 15 December 2017; Accepted Date: 28 December 2017; Published Date: 04 January 2018
Citation: El-Badrawy A, Gadelhak B, El-Badrawy MK, El-Etreby SA, Emarah Z, et al. (2018) Hepatocellular Carcinoma with Endobronchial Metastasis: A Case Report. Vol. 2 No. 1: 1.
Copyright: © 2018 Badrawy AE, et al. This is an open-access article distributed under the terms of the creative Commons attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Keywords
Hepatocellular carcinoma; Endobronchial metastasis; Multidetector computed tomography (MDCT)
Introduction
Endobronchial metastases (EBM) secondary to extrapulmonary solid malignancies are seen rarely. In an autopsy series, only 2% of the cases of extra-pulmonary solid malignant tumors were found to have EBM [1]. A variety of extrathoracic tumors has a tendency to EBM; especially breast, colon, and renal carcinomas are most frequent reported tumors [2,3]. In this report, we represent a very rare case of hepatocellular carcinoma with endobronchial metastasis.
Case Presentation
A 63-years-old woman was admitted to the hospital with a 4-week history of cough, shortness of breath, and abdominal pain. The patient had a history of radio-frequency ablation of hepatocellular carcinoma 1 year previously. Clinical examination and laboratory tests at admission revealed normal findings, including liver function tests, Alpha fetoprotein and serum creatinine. Plain x-ray chest was done. Abdominal ultrasonographies with color Doppler were done. The patient underwent triphasic computed tomography (CT) of the chest, abdomen, and pelvis using a 64 multi-detector CT scanner (Brilliance 64; Philips Healthcare, Best, The Netherlands). Virtual bronchoscopy was done. Tru-cut biopsy was taken from hepatic focal lesions. Bronchoscopic evaluation and biopsy were taken from lung mass. After confirmation of endobronchial metastasis from hepatocellular carcinoma; patient refuses chemotherapy or interventional treatment. She underwent supportive therapy. She died after 11 months from discovering metastatic hepatocellular carcinoma.
Imaging findings
Ultrasonography reveals heterogeneous hepatic focal lesion. MDCT shows right lower lobar pulmonary mass invades the right pulmonary vein and right lower bronchus. The mass has speculated margins (Figure 1). Virtual bronchoscopy reveals obstructed right lower bronchus (Figure 1). Liver shows a welldefined hypodense focal lesion. It shows enhancement in arterial phase, washout in portal and delayed phases. These findings are characteristic of HCC (Figure 1). There is no similar enhancement of the pulmonary or hepatic masses. Bronchoscopy revealed right lower bronchus mass and multiple bronchoscopic biopsies were taken. Bronchoscopic biopsy revealed hepatocellular carcinoma. Final diagnosis was hepatocellular carcinoma with endobronchial metastasis.
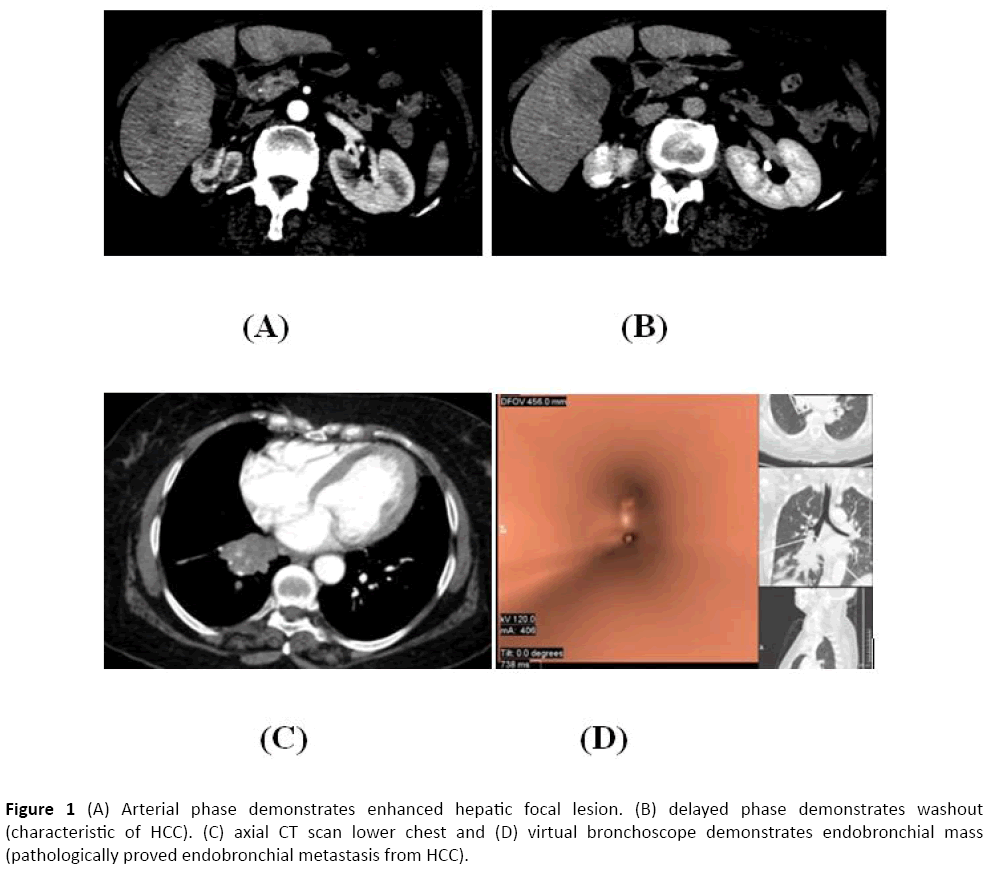
Figure 1: (A) Arterial phase demonstrates enhanced hepatic focal lesion. (B) delayed phase demonstrates washout (characteristic of HCC). (C) axial CT scan lower chest and (D) virtual bronchoscope demonstrates endobronchial mass (pathologically proved endobronchial metastasis from HCC).
Discussion
The endobronchial metastasis of hepatocellular carcinoma is an extremely rare phenomenon [4]. Symptoms and radiological findings are not distinguishable from those of primary lung cancer, and their bronchoscopic presentations are also similar to primary bronchogenic carcinoma. Cough, dyspnea and hemoptysis are the most frequent symptoms in patients with EBM [1]. This coincides with our case as endobronchial metastasis was solitary central lung mass with speculated margin and our case presented with cough and shortness of breath. The computed tomography scan of the chest reveals the most common presentation of EBM is lung mass and the most affecting is right lung [5]. It is unclear why endobronchial metastasis is more frequently found in the right bronchial tree.
The radiological imaging methods as X-ray, computed tomography and magnetic resonance, are nonspecific for distinguishing endobronchial metastases from primary lung carcinoma. The most valuable diagnostic tool is bronchoscopy. It is difficult to differentiate between diagnosis of primary lung carcinoma and EBM on the basis of the symptoms and radiographic findings alone [6]. This agrees with our case as patient presentation suggests primary bronchogenic carcinoma. A total of eighteen patients were identified as having EBM from extrapulmonary malignancies. Among them, twelve patients were women (66.7%) [5]. these coincide with our result.
CT has long been a mainstay of liver and HCC imaging for both initial tumor characterization and post treatment followup for response assessment [7]. This is in agreement with our study.
Multidetector computed tomography (MDCT) and virtual bronchoscopy accurately evaluate the endobronchial metastasis. This is in agreement with other studies [8,9]. Multidetector computed tomography (MDCT) with multiplanar reformates have improved evaluation of bronchial lesion. It accurately evaluates vascular encasement and pericardial invasion. It orients the endoscopist towards the endobronchial masses and assess the extension [8,9].
Conclusion
EBM from extrathoracic malignancies were rare. Fiberoptic bronchoscopy should be performed in all patients with extrapulmonary tumor, who are suspected to have endobronchial metastasis to differentiate it from the primary lung cancer. It should be taken into consideration especially when the patient with previous history of hepatocellular carcinoma.
References
- Katsimbri PP, Bamias AT, Froudarakis ME, Peponis IA, Constantopoulos SH, et al. (2000) Endobronchial metastases secondary to solid tumors: report of eight cases and review of the literature. Lung Cancer 28: 163-170.
- Marchioni A, Lasagni A, Busca A, Cavazza A, Agostini L, et al. (2014) Endobronchial metastasis: an epidemiologic and clinicopathologic study of 174 consecutive cases. Lung Cancer 84: 222-228.
- Akoglu S, Uçan ES, Celik G, Sener G, Sevinç C, et al. (2005) Endobronchial metastases from extrathoracic malignancies. ClinExp Metastasis 22: 587-591.
- Szumera-Ciećkiewicz A, Olszewski WT, Piech K, Głogowski M, Prochorec-Sobieszek M (2013) Endobronchial metastasis from hepatocellular carcinoma – a case description with literature review. Int J ClinExpPathol 6: 1942-1947.
- Kim J, Min D, Song S, Lee J, Jeong H, et al. (2013) Endobronchial Metastases from Extrathoracic Malignancies: Recent 10 Years' Experience in a Single University Hospital. TubercRespir Dis (Seoul) 74: 169-176.
- Öztürk A, Aktaş Z, Yilmaz A (2016) Endobronchial metastasis of mixed germ cell tumors: two cases. TuberkToraks 64: 175-178.
- Choi JY, Lee JM, Sirlin CB (2014) CT and MR imaging diagnosis and staging of hepatocellular carcinoma: Part I. Development, growth, and spread: Key pathologic and imaging aspects. Radiology 272: 635-654.
- Grenier PA, Beigelman-Aubry C, Brillet PY, Lenoir S (2009) Bronchial diseases: CT imaging features. J Radiol 90: 1801-1818.
- Higashino T, Ohno Y, Takenaka D, Watanabe H, Nogami M, et al. (2005) Thin-section multiplanar reformats from multidetector-row CT data: utility for assessment of regional tumor extent in non-small cell lung cancer. Eur J Radiol 56: 48-55.

