Chintale SG*, Kirdak VR, Jatale SP, Shaikh K and Sajit S
Department of ENT, Indian Institute of Medical Science and Research, Maharashtra University of Health Sciences, India
*Corresponding Author:
Chintale SG
Associate Professor
Department of ENT
Indian Institute of Medical Science and Research
Maharashtra University of Health Sciences
Badnapur, Jalna, India
Tel: 919970323030
E-mail: Drsamchinto@gmail.com
Received Date: October 24, 2017; Accepted Date: November 30, 2017; Published Date: December 10, 2017
Citation: Chintale SG, Kirdak VR, Jatale SP, Shaikh K, Sajit S (2017) Fantastic Course of Migratory Metallic Foreign Body and Its Removal. J Ora Med Vol.1 No.1:10
Keywords
Foreign body; Metallic object; Neck
Introduction
Migratory movement of foreign body from the hypo pharynx to the superficial surface of neck is uncommon event. We came across a case of a 55-year-old female who accidentally swallowed a metallic wire as foreign body which was not detectable on our routine oesophagoscope and direct laryngoscopy in Operation Theater under GA. Then we thought that foreign may have migrated to the superficial part of the neck. We decided that proper evaluation of the case with aero digestive tract foreign body is crucial to avoid lethal fatal complications. These types of foreign body like Fish bones are the most commonly ingested foreign body. They may get stick in to the pharynx base of tongue anterior pillars tonsillar surface and mucosal layer of the gastrointestinal tract due to their linear shape and sharp edges, and can then cause serious complications if left untreated. In most of the cases, sharp foreign body like fish bones, chicken bone piece, metallic objects can be removed safely by direct 70 degree laryngoscope if they get stuck in to base of tongue tonsil lingual surface anterior pillars of tonsils, but few of them may migrate extraluminally to the surface skin of the neck in rare cases [1].
Case Report
A 55-year-old female presented to us with painful swallowing and swelling over left side of neck following history of ingestion of a metallic foreign body while eating food in hurry since 7 days. Examination of the oral cavity shows mild inflammatory changes in posterior pharyngeal wall. An attempt to visualize the cricopharynx and larynx by 70 degree scopy was unsuccessful because the patient had excessive cough reflex and uncomfortable to do examination on seating position. Patient have advised USG neck to rule out any neck abscess but USG show there was inflammatory swelling over left thyroid region anterior to left sternocleidomastoid no evidence of any fluid collection or abscess. We started patient with I. V. Antibiotics and analgesic to reduce the swelling and advised CT neck to rule out deep neck space abscess and thyroid inflammation to confirm what the exact pathology is. CT scan reported evidence of metallic foreign body approximately 33 mm which was placed obliquely in post cricoid area toward left side from midline as shown in Figure 1.
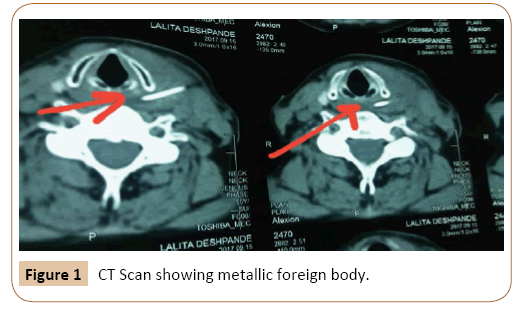
Figure 1: CT Scan showing metallic foreign body.
The patient was then posted for direct endoscopy examination in the form of oesophagoscopy and bronchoscopy and removal of the foreign body under general anesthesia by doing all routine blood investigation which were normal in range. We firstly attempted by use of direct laryngoscopy and then tried by using adult size oesophagoscopy to visualize foreign body under vision we tried it twice but attempt were unsuccessful there was only mucosal ulceration on left side of cricopharynx so we decided to remove foreign body by external neck approach Figure 2.
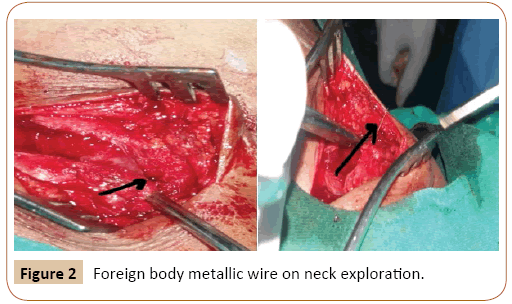
Figure 2: Foreign body metallic wire on neck exploration.
This foreign body was found to be metallic wire approx. 33 mm it was black thin wire as shown in Figure 3. Then the patient was discharged on the 5th day of operation with a 10 days course of antibiotics. On follow-up period clinically the patient was asymptomatic.
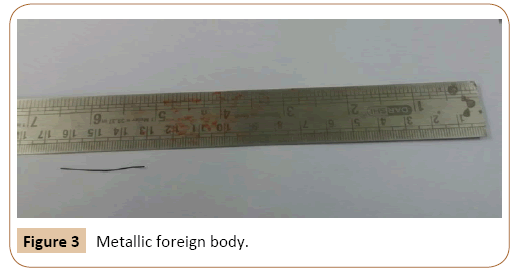
Figure 3: Metallic foreign body.
Discussion
Ingested foreign bodies are most commonly encountered challenging emergency in the Ent field they have been faced by all ENT clinicians. Many of the time, the foreign body gets lodged at the tonsil or the base of tongue [2]. An unnoticed foreign body will usually spontaneously pass out through the gastrointestinal tract without any complication. Spontaneous passage is usually related to the different size and type of the foreign body [3]. Fish bones are the most commonly ingested foreign body in our regional areas like Asian countries [1,4]. They have a tendency to lodge in the posterior pharynx and mucosal layer of the gastrointestinal tract due to their linear shape and sharp edges, and can then cause serious complications if left untreated.
Migration of ingested foreign bodies is very rare in previous reported study they studied Twenty-four patients were reported with migration of foreign bodies within six years in Singapore [1,5]. The largest reported series was of 1088 cases of foreign body ingestion in China in caparison to all of these previous studies [3]. Most of the foreign bodies were reported to be lodged in the pharynx, esophagus, stomach, and duodenum. A sharp foreign body like fish bone, metallic wires has the ability to migrate to the surrounding structure in the neck like thyroid gland, carotid artery, mediastinum, or subcutaneous tissue due to the constant physiological activity of contraction and relaxation of the pharyngeal musculature, esophageal peristalsis, and surrounding tissue reactions [6-9].
Although plain x-ray is a simple and most important investigation to show the presence of radio opaque foreign body, Compute tomography imaging helps to detect the exact location of the impacted foreign body and thus allows for predicting and avoiding any possible complications, especially in the case of migration. In our case, it was necessary to do the computed tomography imaging prior to the surgery to assess the location of the impacted foreign body and its relation to the vital structures of the neck and avoid other possible fatal complications. An extra luminal foreign body has tendency to cause serious complications such as esophageal perforation, per esophageal abscess, retropharyngeal abscess, mediastinitis, arterioesophageal fistula, tracheoesophageal fistula, and carotid rupture. We managed to remove the fish bone from the subcutaneous tissue by making an adequate incision in the skin on left lateral side of neck after confirmation of the location of the metallic foreign body.
Conclusion
Foreign body ingestion is emergency should be managed as early as possible to prevent fatal and serious complications. It is important to ENT surgeon carefully examine the patient with a foreign body in the grave yard of oral cavity like at base of tongue, tonsil lingual sulcus floor of oral cavity and grave yard of larynx especially pyriform fossa lingual surface of epiglottis especially a fish bone, metallic sharp objects like staple pin, screw, nails, wires which has not been found or has been missed by routine oral on repeated examination or endoscopic examination under general anesthesia.
Acknowledgements
This case is reported at our institute Indian Institute of Medical Science and Research, Dist. Jalna thanks to our teachers and colleague for supporting this case report making. Ethical committee permission and patient consent taken.
Source of support
None.
Conflict of interest
None.
References
- Chee LW, Sethi DS (1999) Diagnostic and therapeutic approach to migrating foreign bodies. Ann Otol RhinolLaryngol108:177-180.
- Pang KP, Tan NG, Chia KH, Tan HM, Tseng GY (2005) Migrating of foreign body into the common carotid artery. Otolaryngol Head Neck Surg132:667-668.
- Li ZS, Sun ZX, Zou DW, Xu GM, Wu RP, et al. (2006) Endoscopic management of foreign bodies in the Upper GI tract: Experience with 1088 cases in China. Gastrointestinal Endosc64:485-492.
- Lin HH, Lee SC, Chu HC, Chang WK, Chao YC, et al. (2007) Emergency endoscopic management of dietary foreign bodies in the esophagus. Am J Emerg Med 25:662-665.
- Pignataro L, Laguardia M, Esposito S, Bosis S, Torretta S, et al. (2009) Migrating of foreign body of the neck as a cause of recurrent febrile lymphadenopathy. Int J Pediatr Otorhinolaryngol Extra 4:169-172.
- Masuda M, Honda T, Hayashida M, Samejina Y, Yumato E (2006) A case of migratory fish bone in the thyroid gland. Auris Nasus Larynx 33:113-116.
- Tang IP, Singh S, Shoba N, Rahmat O, Shivalingam S, et al. (2008) Migrating of foreign body into the common carotid and internal jugular vein. Auris Nasus Larynx 3:380-382.
- Bilish DP, Rajan GP, Farooque F (2008) Fish bone migration through the cervical spine. Otolaryngol Head Neck Surg138:407-408.
- Persaud RA, Sudhakaran N, Ong CC, Bowdler DA, Dykes E (2001) Extraluminal migration of a coin in the esophagus of a child misdiagnosed as asthma. Emerg Med J18:312-313.