Berendsen L1*, Bouman DE2 and Venneman NG1
1Department of Gastroenterology and Hepatology, MST Enschede, The Netherlands
2Department of Radiology, MST Enschede, The Netherlands
*Corresponding Author:
Berendsen L
Department of Gastroenterology and Hepatology
MST Enschede, The Netherlands
Tel: (053) 487 2410
E-mail: L.Berendsen@mst.nl
Received date: February 06, 2017; Accepted date: April 19, 2016; Published date: April 22, 2016
Citation: Berendsen L, Bouman DE, Venneman NG. Duodenal Diverticulitis Presenting as Cholangitis. J Clin Gastroenterol Hepatol 2017, 1:2. doi: 10.21767/2575-7733.1000014
An Endoscopic Retrograde Cholangiopancreatography (ERCP) was performed because of suspected ascending bacterial cholangitis due to common bile duct stones. A prominent papilla with an abnormal aspect was noticed. Given the suspicion of a malignancy, a CT-abdomen and additional gastroduodenoscopy were performed for further analysis. These resulted in the final diagnosis: duodenal diverticulitis, which apparently mimicked ascending bacterial cholangitis. Conservative treatment with supportive care resulted in full recovery.
Keywords
Cholangitis; Duodenal obstruction; Gallstones
Case Presentation
A 90-year-old female patiënt was referred to our hospital with suspicion of ascending bacterial cholangitis due to common duct stones. Her medical history reported breast cancer and a recent admission to another hospital because of cholangitis, from which she quickly recovered after intravenous antibiotics.
Her main complaints were nausea and loss of appetite. In addition, she experienced an unpleasant taste in her mouth. Blood tests showed elevated liver enzymes (Alkaline Phosphatase: 734 U/L, gamma-Glutamyl Transpeptidase: 2003 U/L, ASpartate Amino-transferase 303 U/L, ALanine Aminotransferase 407 U/L, bilirubin: 47 μmol/L; all 3 × upper limit of normal) and elevated C-reactive protein. Abdominal ultrasound, performed in another hospital, showed a dilated common bile duct of which the distal part could not be examined. Another finding was the presence of multiple gallbladder stones.
Discussion
Suspecting recurrent ascending bacterial cholangitis due to bile duct stones, an Endoscopic Retrograde CholangioPancreatography (ERCP) was performed. The major papilla was bulging, but not due to the classic configuration of an impacted gallstone. Despite of a small pre-cut papillotomy, canulation of the common bile duct was not achieved. Given the suspicion of malignancy, an abdominal CT-scan was performed. This showed a large juxtapapillairy diverticulum with massive air in the common bile duct. No other abnormalities were seen in papillar or pancreatic region (Figure 1). Additional linear gastroscopy showed a diverticulum, localized proximal of the major papilla, from which pus was dripping. The cavity of the diverticulum showed hyperaemic mucosa with fibrinous tissue.
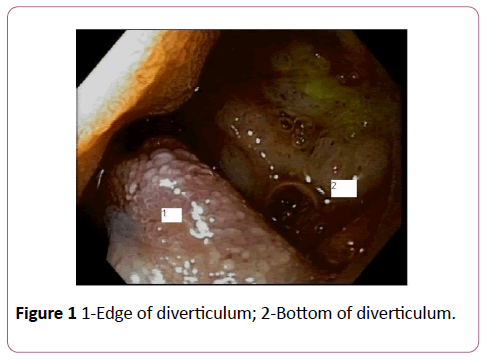
Figure 1: 1-Edge of diverticulum; 2-Bottom of diverticulum.
Conclusion
We concluded therefore that our patient suffered from duodenal diverticulitis (Figure 2), a disorder, althouh rare, that has been reported previously [1,2]. Recurrent cholangitis with massive common bile duct air was probably caused by perforation of the diverticulum into the common bile duct. Several days after admission, with only supportive care, our patient was released from the hospital with a further uneventful course.
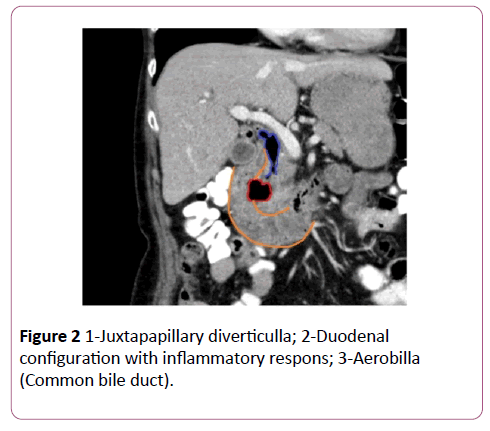
Figure 2: 1-Juxtapapillary diverticulla; 2-Duodenal configuration with inflammatory respons; 3-Aerobilla (Common bile duct).
There is another case-report of a patient suffering from cholangitis caused by an ampullary duodenal diverticulum in which the surgical treatment consisted of choledochojejunostomy utilizing a Roux-en-y-loop [3]. Our case showed that antibiotic treatment and supportive care may be sufficient.
References
- De Perrot T, Poletti PA, Becker CD, Platon A (2012) The complicated duodenal diverticulum: Retrospective analysis of 11 cases.Clin Imaging36:287-294.
- Luz LP, Eloubeidi MA (2009) Duodenaldiverticulitismimickingcholangitis: Endoscopic and EUS appearance. Am J Gastroenterol104:2125-2126.
- Castilho Netto JM, Speranzini MB (2003) Ampyllarydudenal diverticulum and cholangitis. Sao Paulo Med J121:173-175.

