Mathew AL1*, Cherian SA2 and Daniel MP3
1Department of Oral Medicine and Radiology, Pushpagiri College of Dental Sciences, India
2Department of Pedodontics and Preventive Dentistry, Pushpagiri College of Dental Sciences, India
3Department of General Surgery, Believers Church Medical College and Hospital, India
*Corresponding Author:
Dr. Anuna Laila Mathew
Associate Professor
Department of Oral Medicine and Radiology
Pushpagiri College of Dental Sciences
Medicity, Perumthuruthy, Tiruvalla
Kerala, India
Tel: +918547431225
E-mail: drmathewdan@yahoo.co.in
Received Date: December 29, 2017; Accepted Date: January 09, 2018; Published Date: January 19, 2018
Citation: Mathew AL, Cherian SA, Daniel MP (2018) A Giant Sialolith in the Submandibular Salivary Gland Parechyma - A Rare Entity. J Ora Med Vol.2 No.1:1
Keywords
Sialolith; Saliva; Submandibular gland; Parenchyma; Xerostomia
Introduction
Saliva is produced from the major and minor salivary glands that are dispersed throughout the oral cavity. The most common cause of swelling of the salivary gland is the presence of salivary calculi obstructing the salivary flow. Sialolith is a calcified organic matter that is formed within the secretory system of the salivary glands. A nidus of the salivary organic material becomes calcified and forms a sialolith. Sialolithiasis is one of the most common diseases of the salivary gland. Around 1% of the world population is affected by this disease [1]. Males are commonly affected as compared to females and in the age group between 30-60 years. Most common location is submandibular gland around 80-90%. Duct is more commonly affected as compared to the parenchyma [2,3]. Sialolith affecting parotid gland is around 6-20% and also in the sublingual and minor salivary glands around 1-2% [1].
The submandibular gland is commonly affected. Higher rate of giant sialolith formation in the gland is due to the tortious course of the Wharton’s duct, high calcium and phosphate levels, and dependent position of the gland which makes it prone to stasis [4]. This is usually associated with pain, inflammation and in some cases pus discharge due to secondary infection. Intraglandular sialolith require submandibular sialadenectomy. Clinical, radiographic examination are required for the correct diagnosis and treatment plan. Here we report an interesting case of a large sized sialolith in the parenchyma of the left submandibular gland.
Case Report
A 52 year old female reported to the Department of Oral Medicine and Radiology with the chief complaint of pain and swelling in the lower left side of the face since one year. The patient had a history of recurrent swelling and pain, for which the patient had taken analgesic and antibiotics following which the patient gets symptomatic relief. Since one week the pain is severe and pus discharge in the oral cavity reported. Pain is severe continuous and radiates to the neck and left side of the face. No increase of pain following the sight of food or xerostomia reported. Patient is a known hypertensive and is not on any regular medication.
Extraoral examination revealed a diffuse swelling on the left side of the face extending from the lower border of the mandible in the region of 36 to around 3 cm inferiorly. Medially from the 36 region and distally around 1 cm anterior to the angle of the mandible (Figure 1). The surface skin appeared normal. On palpation it was hard in consistency, fixed and non-tender on palpation. Intraoral examination revealed no obvious swelling except for an exophytic growth with pus discharge on manipulation (Figure 2).

Figure 1: Extra oral photograph.
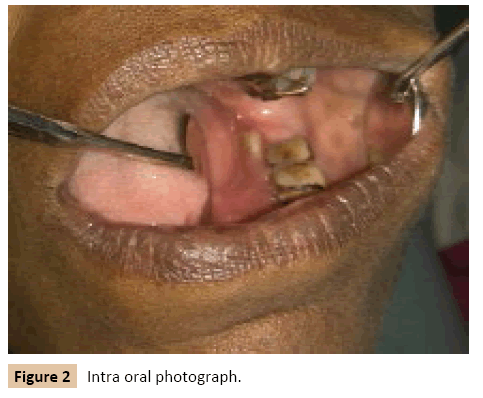
Figure 2: Intra oral photograph.
A provisional diagnosis of an infected left submandibular sialolith was made. Panoramic radiograph was advised that revealed a large radiopaque mass within the substance of the gland measuring around 4 × 4 cm (Figure 3). Cropped image of the panoramic radiograph represented in Figure 4. Patient was advised to undergo a total surgical excision of the gland extra orally under general anesthesia. An incision was placed around in the skin crease 2 cm below the lower border of the mandible. Sialoadectomy was performed under general anesthesia, and the entire submandibular gland along with a white colored sialolith was removed from the parenchyma of the gland measuring around 3 × 4 cm. The calculus was round and had an irregular surface. The postoperative period was uneventful with healthy healing of the surgical site.
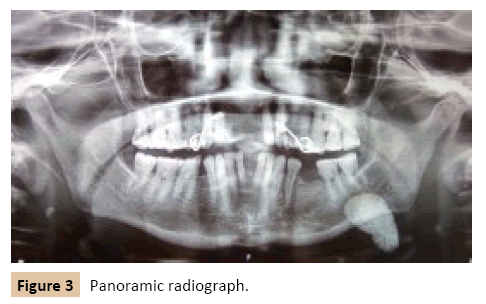
Figure 3: Panoramic radiograph.
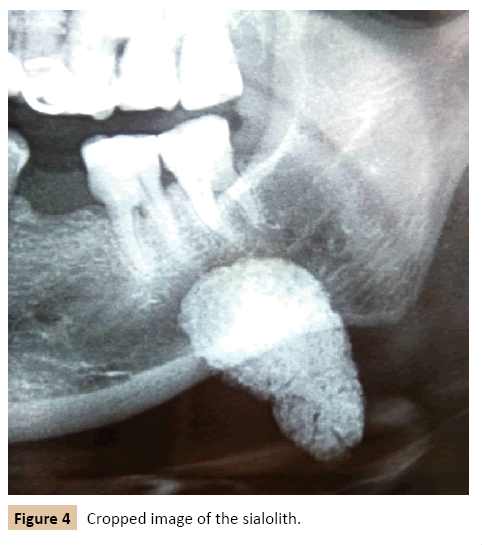
Figure 4: Cropped image of the sialolith.
Discussion
Sialolith is one of the most common cause of salivary obstruction it is characterized by pain, inflammation and occasionally associated with pus discharge. Size of the Sialolith ranges from small particles to giant sialoliths. Salivary calculi are usually found in the ducts and sialolith in the parenchyma occurs in only 9-17% of cases [5,6]. Salivary glands with sialoliths are usually enlarged and tender. The majority of the sialoliths are formed from phosphate and oxalate salts. They are also composed of varying ratios of organic and inorganic substances [7]. The organic substances are glycoproteins, mucopolysachrides and cellular debris, inorganic substances are mainly calcium carbonate and calcium phosphate. Sialoliths are ovoid or round and yellowish in color. Complications from sialolith include acute sialadenitis, ductal stricture, ductal dilatation and recurrent infections.
Gaint sialoliths are a rare finding their size varies from approximately from 1.5 cm-7 cm. The clinical and radiographic methods for diagnosis includes conventional radiographs like occlusal and panoramic radiographs, sialography, ultrasound and computed tomography. Submandibular gland calculi is radiopaque in 80-94% of cases [8-10]. Ultrasonography is widely reported to be useful in detecting salivary stones. As many as 90% of all stones larger than 2 mm can be detected ultrasonographically [11]. The characteristic ultrasound reveals an echo reflection with marked dorsal sound shadowing. Computed tomography is also highly diagnostic [12].
Submandibular sialoliths are usually removed surgically either via intraoral or extra oral approach. In instances when the sialolith is small and are located near the ductal orifice it can be removed by widening the ductal orifice using a lacrimal probe. In the case of large sialolith affecting the gland parenchyma should be treated with surgical removal of the gland via extra oral approach.
Conclusion
In the present case our patient presented with typical clinical and radiographic findings and sialadenectomy was performed was the treatment plan due to the location of the gland. The present case illustrates the need for proper diagnosis and treatment of choice in the case of salivary gland diseases. Post-operative follow up is essential to ensure that the patient is symptom free and stone free long term. To conclude clinical and radiographic findings are important in determining the precise location and size of the sialolith in order to indicate the right treatment for the patient.
References
- Andretta M, Tregnaghi A, Prosenikliev V, Staffieri A (2005) Current options in Sialolithiasis diagnosis and treatment. Acta Otorhinolaryngol Ital 25: 154-149.
- Grases F, Santiago C, Simonet BM, Costa-Bauza A (2003) Sialolithiasis: mechanism of calculi formation and etiological factors. Clin Chim Acta 334: 131-136.
- Austin T, Davis J, Chan T (2004) Sialolithiasis of submandibular gland. J Emerg Med 26: 221-223.
- Burket LW, Grenberg MS, Glick M, Ship JA (2008) Burket’s Oral Medicine. (11thedn), BC Decker.
- Lustmann J, Regev E, Melamed Y (1990) Sialolithiasis: A survey on 245 patients and a review of literature. Int J oral Maxillofac Surg 19: 135-138.
- Zenk J, Koch M, Klintworth N, Koing B, Konz K, et al. (2012) Sialendoscopy in the diagnosis and treatment of Sialolithiasis: A study on more than 1000 patients. Otolaryngol Head Neck Surg 147: 858-863.
- Turner MD (2009) Sialoendoscopy and salivary gland sparing surgery. Oral Maxillofacial Surg Clin N Am 16: 149-163.
- Zakaria MA (1981) Giant calculi of the submandibular salivary gland. Br J Oral Surg 19: 230-232.
- Marchl F, Kurt AM, Dulgerov P, Lehmann W (2001) Retrograde theory in Sialolith formation. Arch Otolaryngol Head Neck Surg 127: 66-68.
- Williams MF (1999) Sialolithiasis. Otolaryngol Clini North Am 32: 819-834.
- Van den Akker HP (1988) Diagnostic imaging in salivary gland diseases. Oral Surg Oral Med Oral Pathol 66: 625-637.
- Weissman JL (1995) Imaging of salivary glands. Semin Ultrasound CT MR 16: 546-568.