Keywords
Persons with cervical cord injury; The process of subjective disability acceptance; The role of nurses and rehabilitation professions; Long-term psychological support; After the acceptance of disability
Introduction
Spinal cord injury is an acquired disability that is generally caused by trauma to the spinal cord in an accident or disaster. The related sensory and motor disorder persists permanently in many cases, even after recovery from a medically critical phase, leading to many difficulties in daily life. Furthermore, patients with spinal cord injury experience significant psychological shock as they are forced to transition from healthy people to people with a disability, losing their physical function, own way of life, and social status.
The following studies have been conducted on patients with spinal cord injury: Berger and Garrett reported the importance of care pertaining to psychological aspects in patients with spinal cord injury [1]; Frank, Van Valin, and Elliott reported the process of adaptation in patients with spinal cord injury [2]; Elliott and Frank reported depression in patients with spinal cord injury [3]; Kim reported that patients with spinal cord injury have various conflicts such as the gap between mental and physical abilities, the gap of physical ability before and after the injury, and the gap in the social status due to these losses before and after the injury [4], and they suggested the importance of psychological stability and long-term adaptation. Thus, patients with spinal cord injury are under unexpected/unpredicted crisis, due to which they have been the focus of research in the area of rehabilitation psychology. However, related research in the area of social psychology is also gaining attention [5].
Research on the psychological aspects of patients with spinal cord injury developed particularly in the U.S. since the 1950s, because many soldiers suffered from physical disabilities in World War II. Additionally, in the field of rehabilitation psychology, studies have been conducted with reference to the psychological aspects of general patients with disability. Gradually, studies that captured the psychological aspects of people with disability from the view of disability acceptance emerged, and Grayson first pointed out the importance of disability acceptance, which started the discussion in the area of rehabilitation [6]. Subsequently, Dembo et al. and Wright revealed the importance of the transformation of value, whereby disability acceptance is facilitated by the patient’s transformation of value [7,8]. Furthermore, from the 1960s to 1980s, the stage theory was proposed, according to which the disability acceptance process occurred in stages. Cohn proposed 5 stages: 1) Shock, 2) Expectancy of recovery, 3) Mourning, 4) Defense, and 5) Adaptation [9]; while Fink proposed 4 steps: 1) Shock, 2) Defensive retreat, 3) Acknowledgement, and 4) Adaptation [10]. Further, several other researchers proposed the presence of different processes from injury to adjustment [11-13]. In Japan, Ueda proposed 5 stages: 1) Shock, 2) Denial, 3) Confusion, 4) Effort to find a solution, and 5) Acceptance [14], and Furumaki reported the process of acceptance of disability [15]. However, the stage theory has been criticized and questions have been raised about whether or not we should follow the conventional disability acceptance stage. Instead, it has been proposed that each individual’s complex process of building a life with a disability should gain attention [16,17]. Thus, the focus of research in this area is gradually shifting from population of people with disability to case studies to gain a deep understanding of individuals’ experiences [18,19]. Furthermore, Nagumo categorized the mental suffering after the injury into self-acceptance and social acceptance, which pertain to tackling the suffering that arises from the patient and from other people, respectively [20]. Overall, the results of such studies indicate that it is important for other people to accept the person with disability from the bottom of their heart.
Hotta and Ichimura discussed acceptance of disability as the process of reviewing previous experiences and engaging in selfreflection, and to realize that others have been able to think positively and accept the disability [21]. Thus, it should be based on the subjective evaluation of the person. Further, the authors expressed discomfort in the fact that other people evaluate the presence of acceptance of disability. Nakajima and Inoue discussed that there is no standardized and common concept for acceptance of disability that can be judged by the society because it pertains to how the person perceives “him/herself” [22]. Furthermore, as the voice of the patient, Shinsha, a physician with cervical cord injury from a rugby game accident, discussed the importance of transformation of value, saying that it may be more appropriate to consider it as an expansion of one’s value since human values may not change so easily only because of a disability [23]. Oshitomi, an occupational therapist who had an intractable neurological disease, discussed acceptance of disability, saying that it may not be about whether or not we accept the disability, but it may be the nearest to saying “working out differences between” the life before and after disability [24].
Therefore, although it is important to evaluate subjective acceptance of disability that the person with cervical cord injury experiences, with a focus on the individual, most reports about the process of subjective disability acceptance in patients with spinal cord injury are limited to patients with thoracic and/or lumbar injury, and few reports have explored the process in patients with cervical cord injury with severe disability and quadriplegia. Furthermore, many studies surveyed until the participants accepted the disability, and few studies have investigated the process after the acceptance of disability has occurred. However, in the clinical practice of rehabilitation medicine, acceptance of disability is considered as “the patient has not accepted the disability,” including having negative behaviors such as “being unmotivated” and “problematic,” and it is sometimes considered as one of the barriers to rehabilitation. Few studies have investigated the acceptance of disability in rehabilitation professions.
The objective of this study was to clarify the process of subjective disability acceptance before and after the acceptance of disability in persons with cervical cord injury and to investigate the role of nurses and rehabilitation professions in this process.
Methods
The participants were 10 males with cervical cord disability living at home. After conducting a questionnaire-based survey on participant characteristics, the main author conducted a semi-structured interview with all the 10 participants. Each interview lasted for about 60 to 120 minutes. The participants’ answers were recorded using an IC recorder, and a verbatim transcript was created after the interview, for analysis. The transcribed data were confirmed with the participants to ensure their reliability.
We identified statements about the participants’ disability after the spinal cord injury from each sentence unit, after which the identified statement was assigned a label. We collected similar labels by reading them to capture the essential meaning of the whole argument and then expressed them in one sentence to create a code. Similarly, we collected similar codes by reading them to capture the essential meaning of the whole argument and then created subcategories. After creating subcategories for all the 10 cases, we identified similar subcategories to create categories. We discussed our analyses with colleagues who were familiar with qualitative research.
In the questionnaire-based survey, we collected information about age, gender, site of injury, age at the time of injury, and family status. In the interview, we asked the participants to freely talk about 1) life before the injury; 2) the injury; 3) hospitalization; 4) the time when they recognized the disability; 5) the time when their perception about disability changed; 6) when they received a disability notification; 7) the time when they received the disability certificate; 8) their feelings about returning to the society; 9) their own disability; 10) their future. Furthermore, we asked them to talk in chronological order from the injury to the present time.
We explained to the participants, both verbally and in written, about 1) the objectives and method of the study, 2) the time required, 3) their right to withdraw from the study at any time, 4) that there would be no harm for rejecting participation and/or withdrawal, 5) the interview would be recorded using an IC recorder, and 6) that individuals would not be identified when the results would be published. Subsequently, we obtained verbal consent for participation.
The research protocol was reviewed and approved by the Ethics Committee of the Kobe University (No.535).
Results
The participants were 10 males, and their age ranged from 28-47 years. The site of injury was C6B2 for 3 participants, C6B3 for 3 participants, C7 for 3 participants, and C8 for 1 participant. The cause of injury was a traffic accident for 7 participants, a pool diving accident for 2 participants, and a sports accident for 1 participant. The average age at the time of injury was 18.0 ± 2.4 years, and the average time since injury was 19.4 ± 6.1 years (Table 1).
| Participant |
Age |
Gender |
Level of injury |
Cause of injury |
Age at injury (y) |
Years post injury |
| 1 |
47 |
Male |
C6B2 |
Pool accident |
15 |
32 |
| 2 |
36 |
Male |
C6B2 |
Pool accident |
17 |
19 |
| 3 |
37 |
Male |
C6B3 |
Traffic accident |
20 |
17 |
| 4 |
40 |
Male |
C7 |
Traffic accident |
19 |
21 |
| 5 |
26 |
Male |
C7 |
Traffic accident |
17 |
9 |
| 6 |
48 |
Male |
C6B2 |
Traffic accident |
23 |
25 |
| 7 |
33 |
Male |
C6B3 |
Sport accident |
15 |
18 |
| 8 |
38 |
Male |
C8 |
Traffic accident |
19 |
19 |
| 9 |
41 |
Male |
C7 |
Traffic accident |
19 |
22 |
| 10 |
28 |
Male |
C6B3 |
Traffic accident |
16 |
12 |
Table 1: Participant profiles.
Based on the survey, we identified statement units regarding the participants’ perception and feelings about their own disability from the time of injury to the present, and extracted them as sentences (Table 2). The sentences were then classified into 23 categories and 62 subcategories (Table 3). These themes represented the participants’ status at each stage of the process of acceptance of disability (Table 4). The details of the categories and subcategories have been described in subsequent sections of this paper, using some examples. The following symbols have been used to identify various components: Category: [], Subcategory: <>, participants’ quotes: “”, Participant No. ().
| Participant |
Label |
Code |
Subcategory |
Category |
| 1 |
197 |
39 |
18 |
18 |
| 2 |
111 |
33 |
13 |
13 |
| 3 |
82 |
28 |
15 |
15 |
| 4 |
138 |
38 |
18 |
18 |
| 5 |
64 |
32 |
17 |
17 |
| 6 |
96 |
38 |
19 |
19 |
| 7 |
101 |
39 |
19 |
19 |
| 8 |
68 |
25 |
10 |
10 |
| 9 |
110 |
46 |
19 |
19 |
| 10 |
84 |
24 |
13 |
13 |
Table 2: Participant statement coding labels with number, code, subcategory, and category.
| Category |
Subcategory |
| Shock |
Torpor |
| Optimism |
| Grief |
Regret |
| Sorrow |
| Disappointment |
| Fret |
Impatience |
| Despair |
Feeling of being estranged |
| Embarrassment for the change |
| Think about death |
| Feeling impotent |
| Incurable conviction |
Notice |
| Rehabilitation |
| Disability certificate |
| Expecting to recovery |
Unarticulated expectation |
| Passivity |
Spiritless |
| Lack of consent |
| Conflict |
Comparison |
| Desire |
| Denial |
| Feeling that the situation is unbearable |
| Repulsion |
Repulsion against others |
| Anger against myself |
| Agony |
Line of sight |
| Inability to be together |
| Relations with others |
| Anxiety |
Anxiety in daily life |
| Anxiety about the future |
| Recognition of the disability |
Recognizing what I cannot do |
| Recognizing being disabled through the disability certificate and the need to use a wheelchair |
| Resignation |
Resignation to environmental obstacles |
| Resignation to the idea that recovery is not likely |
| Hope |
Possible to move freely |
| Want to be like this person |
| Effort |
Advance forward |
| I can do it |
| Self-efficacy |
| Adaptation |
Do not mind wheelchairs |
| I can live |
| I can go out |
| Goal |
Goal for life |
| Thought of being at home |
| Goal for activities |
| Role in the society |
| Existence of others |
Not alone |
| I had help |
| No actual feeling of the disability |
No negative feeling about having a disability certificate |
| A disability certificate is the same as a driver’s license |
| Acceptance |
No feeling of being disabled |
| Acceptance of disability |
| No regret |
| Lack of acceptance |
I may not do it |
| I do not accept it completely |
| I want to go back to being a healthy person |
| Live positively |
Being true to oneself |
| I want to enjoy my life |
| Thinking positively |
| I want to aim for the best |
| I want to help |
| Worry |
Worry about the future |
| Worry about the body |
| Worry about one’s economic status |
Table 3: Category and subcategory.
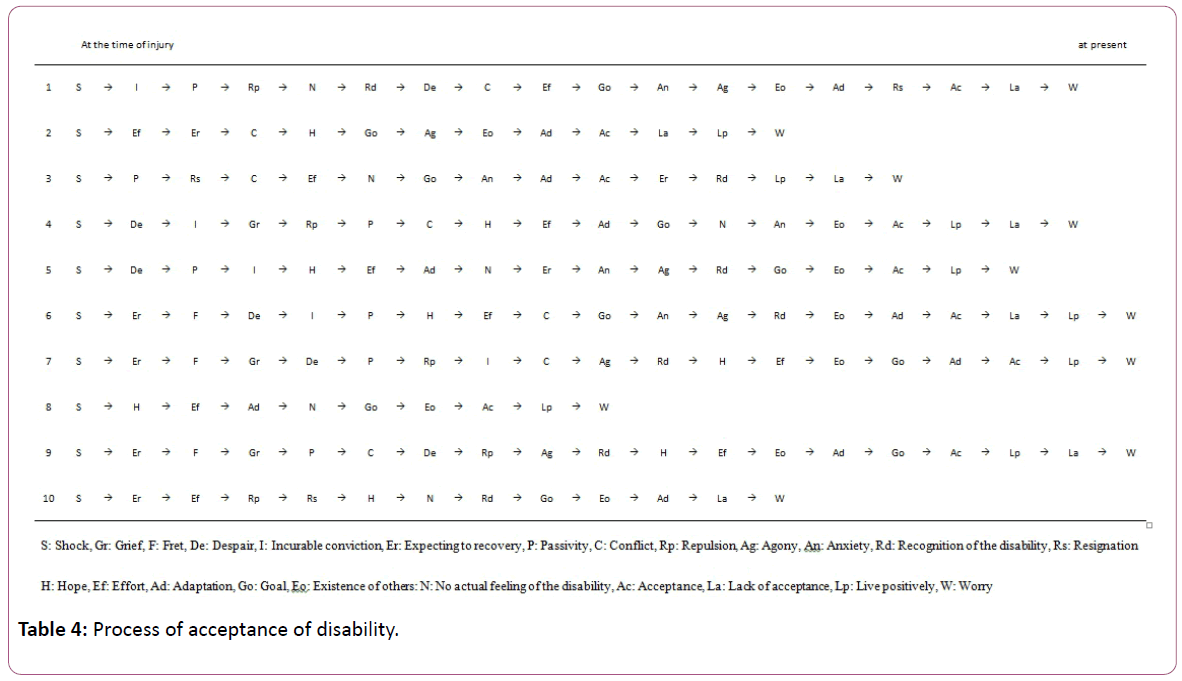
Table 4: Process of acceptance of disability.
[Shock]
This category pertained to the state of psychological shock after the injury. It was experienced by all the 10 participants. The subcategories were and .
was represented by statements such as, “I did not have a sense of reality that my body did not move” (1), “Even though I was informed about the cervical cord injury, I didn’t understand it” (2), “I didn’t think about the inability to move” (3), “My body didn’t move at all. I wondered whether it will be cured” (4), “I thought something was wrong since my body did not move” (5), “I did not understand what happened. I thought that this is how one feels when there are bruises all over the body” (6), “I thought that it was because of the anesthesia” (7), “I didn’t know exactly what is happening” (9), and “I did not know what had happened to me” (10).
was expressed through statements such as, “I expected that I would walk to home tomorrow” (8).
[Grief]
This category represented the state of sadness and sorrow experienced after the injury. It was seen in 3 people— Participant 4, 7, and 9. The subcategories were , , and .
was expressed in statements such as, “I regret that I didn’t follow the traffic rules” (4).
was evident from the statement, “I was shocked since I could not to anything by myself” (7).
was reported through statements such as, “I thought there is no hope in my life” (9).
[Fret]
This category involved the situation that led to fretting because of the feeling that the situation would remain this was and it would not improve. It was reported by 3 people— Participant 6, 7, and 9. The subcategory was .
was evident from statements such as, “I thought that the situation did not get better. I wondered if this would remain the same and that I would have to spend the rest of my life staring at the ceiling” (6), “I noticed that I could not move” (7), and “I started to wonder what if my body does not move” (9).
[Despair]
This category involved a feeling of anxiety regarding the future, and feelings of ineffectualness and confusion. It was observed in the statements of 6 respondents—Participant 1, 4, 5, 6, 7, and 9. The subcategories were , , , and .
was represented by statements such as, “Excessive thinking was the most tiring” (1).
was expressed as follows: “It was the moment when I thought that I could never play soccer again, (it was) a great shock” (4).
was evident from statements such as, “I thought that I want to die. I despaired over life because of the injury” (5), “When I saw my disability certificate, I asked a housemaid to stab me” (6), and “I wondered in what way I could die” (9).
was expressed as follows: “It was a feeling of being kept alive” (7).
[Incurable conviction]
This category was the state of being convinced that the cervical cord injury is incurable. It was seen in 5 people— Participant 1, 4, 5, 6, and 7. The subcategories were , , and .
was expressed in statements such as, “My doctor told me that it would not be cured, so I thought the same” (1), “I was told by a doctor that it will not to be cured and I thought that I will be bedridden for life” (4), and “My doctor told me that I would remain bedridden, and I thought it would not be cured” (6).
was evident from statements such as, “I was actually trying to walk but I couldn’t, and I thought that I may be unable to walk as expected” (5).
was expressed in statements such as, “I thought that it is incurable when I got a disability certificate” (7).
[Expecting to recover]
This category was the state in which it was thought that the cervical cord injury would improve. It was seen in 6 people— Participant 2, 5, 6, 7, 9, and 10. The subcategory was .
was expressed in statements such as, “I thought that I had improved even if not completely cured” (2), “Although unreasonable, I thought that the situation might change a little” (3), “I thought that I might improve a little even if I could not walk” (5), “I thought that I would be able to go home at the end of the month since my body did not move just because of the bruises I had all over the body” (6), “I expected that it would get better soon and that I would gradually recover” (7), “I had a positive thought that I would be able to go out with my friends again sometime” (9), and “I thought that it might be still cured even though I received a notice from my doctor” (10).
[Passivity]
This category involved the situation of not acting by oneself with reference to rehabilitation efforts and daily life. It was seen in 7 people—Participant 1, 3, 4, 5, 6, 7, and 9. The subcategories were and .
was expressed in statements such as, “I felt I was being indifferent” (1), “I only did what I was told to” (3), “I disliked the rehabilitation sessions and did not readily do it by myself” (4), “I only did as I was told to” (5), and “I did not engage in rehabilitation activities based on my own initiative” (7).
was expressed in statements such as, “I did not feel like working hard if others did not have to” (6) and “I was wondering why I had to do such a thing” (9).
[Conflict]
This category involved a state of strong psychological tangle stemming from comparing one’s situation with that of others. It was seen in 7 people—Participant 1, 2, 3, 4, 6, 7, and 9. The subcategories were , , , and .
was expressed in statements such as, “A person in the same state as mine did not have any problem at all and was able to move to a bed by him/herself” (1), “I compared myself with other people with cervical cord injury as to what height they could get to with a transfer motion” (3), “I watched people of the same level of disability” (4), and “I watched around” (6).
was evident from, “After looking at the transfer motion in other persons with cervical cord injury, I started to feel that I wanted to do this as well and as soon as possible” (2).
was expressed as, “I did not want to admit that I had become a person with disability” (7).
was expressed as, “I thought to myself, ‘why do I need to have such a life’” (9).
[Repulsion]
This category was the state where the patient experienced anger and resisted against others and against one. It was seen in 5 people—Participant 1, 4, 7, 9, and 10. The subcategories were and .
was expressed through statements such as, “I felt, “Why should I do such a thing?” I cried and returned to my room” (1), “I rebounded on a nurse in charge” (4), and “I felt annoyed and vented my anger on others” (9).
was reported as, “I was frustrated with myself because I could not move” (7) and “I was frustrated because there was no solution” (10).
[Agony]
This category represented the state in which relations with others suffered. It was seen in 6 people—Participant 1, 2, 5, 6, 7, and 9. The subcategories were , , and .
was expressed in statement such as, “I was worried about being seen by others” (1), “It felt great to get a glance of others” (2), and “I was ashamed to be seen in a wheelchair” (7).
was expressed as, “I wanted to attend an athletic meet together” (5).
was expressed as, “Stress piled up and I quarreled with my mother” (6) and “I was annoyed with a therapist and experienced self-hate” (9).
[Anxiety]
This category was the state of feeling anxiety about life and about the future. It was seen in 5 people—Participant 1, 3, 4, 5, and 6. The subcategories were and .
was expressed through statements such as, “I was anxious about going home, although I was able to do it” (1) and “I continually lived with anxiety” (4).
was reported as follows: “I thought about what I would do when I went home” (3), “I wondered if I could attend high school” (5), and “Because I did not have anything particular to do when I went home, I thought whether I should stay indoors” (6).
[Recognition of the disability]
This category was the state of recognizing one’s disability. It was seen in 6 people—Participant 1, 5, 6, 7, 9, and 10. The subcategories were and .
was expressed as follows: “I recognized fully for the first time that I could not move” (1), “I thought that I would not be able to live in my hometown again” (5), “I liked to go outside, but I could not get out (6), and “I experienced the disability when I failed to go to the restroom” (10).
was expressed in statements such as, “When I received a disability certificate, I realized being disabled” (7) and “When I sat in a wheelchair, I thought that I had become a person with a disability” (9).
[Resignation]
This category pertained to the state involving a feeling of ineffectualness due to limited actions because of the disability, and the disability not being cured. It was seen in 3people— Participant 1, 3, and 10. The subcategories were , and .
was expressed as, “Though I wanted to go out, I may never do so” (1).
was evident from statements such as, “When it was said that I had not improved even though half a year had passed, I thought that there was no solution for it” (3) and “When I understood that it will not be cured, I felt resigned” (10).
[Hope]
This category was the state of finding hope in living as a person with cervical spinal cord damage, and feeling in condition to change forward. It was seen in 8 people—Participant 2, 4, 5, 6, 7, 8, 9, and 10. The subcategories were and .
was expressed in statements such as, “I can go where I want using a wheelchair” (2), “I thought that I can go anywhere with a wheelchair” (5), “I was able to move freely with a wheelchair, and movement became easier” (7), “I was invited to go out to play” (8), “I became able to move freely with a wheelchair” (9), and “I became free after I was able to get on the wheelchair” (10).
was expressed as, “Looking at a person with the same cervical spinal cord injury as mine, I thought I want to be like this person” (4) and “I thought I want to put the bowl on my palm and eat the beef bowl like that person with cervical cord injury” (6).
[Effort]
This category was the state of making an effort despite the disability. It was seen in all the 10 participants. The subcategories were , , and .
was expressed as, “I started to work on transfer practice more seriously” (1), “It was interesting to move” (2), “I ran on the wheelchair training rollers, then I ran outside and ran earnestly” (3), “I did my best because I hated that I could not do it because I had become disabled” (5), “I met people with cervical cord injury and worked hard on rehabilitation” (6), “I tried hard to do my own things by myself” (7), “I wanted to go out to play and therefore I worked hard on rehabilitation” (8), and “Since I died once, I tried to make a mark before I die” (9).
was expressed as, “It is heartbreaking but I am still doing the things I can do by myself” (4).
was expressed as, “I felt motivated when I could use my muscular strength, and when my ability to do things increased” (10).
[Adaptation]
This category pertained to the state of thinking positively about living as person with spinal cord injury. It was seen in all the 10 participants. The subcategories were , , and .
was evident from statements such as, “I stopped being worried about a wheelchair” (1), “I did not feel that others’ eyes were on me” (3), “I did not dislike myself in the wheelchair” (7), “I became able to meet my friends using the wheelchair” (9), and “I was not worried about being seen by others” (10).
was expressed as, “I thought I can live in such a body” (2), “I thought that I could live as a person with a disability” (4), and “I thought I can enjoy in a wheelchair” (8).
was expressed as, “I became able to go out” (5) and “I became able to go anywhere on a train” (6).
[Goal]
This category represented the state of imagining a goal and a role in one’s future. It was seen in all the 10 participants. The subcategories were , , , and .
was expressed as, “I thought that I wanted to move to a bed by myself” (1).
was expressed as, “The goal was to be able to live alone” (2), “I thought of only one thing—about going home” (3), “The final goal was to go home” (6), “I wanted to be able to live alone” (7), and “The feeling of wanting to go home was strong” (10).
was “I wanted to engage in sports and travel” (4) and “I wanted to drive a car” (9).
was expressed as, “I thought that I should work” (5) and “I thought that one should work to be able to live alone” (8).
[Existence of others]
This category pertained to the state of realizing the existence of others in terms of receiving their support and help. It was seen in 9 of the 10 participants, excluding Participant 3. The subcategories were and .
was expressed through statements such as, “It is a big matter that I am not alone” (1), “I was not disappointed that I was alone” (9), and “There is a person with the same cervical cord injury around me” (10).
was evident from statements such as, “It was helpful to have a friend” (2), “I pushed forward to return home to be able talk to various people” (4), “Because of parents’ support, I was able to do my best” (5), “A teammate was taught how to load the wheelchair” (6), “Though I could not do it by myself, I had various people to help me” (7), and “I met a lot of people; I got help” (8).
[No actual feeling of disability]
The category was the state of not actually feeling one’s disability. It was seen in 6 people—Participant 1, 3, 4, 5, 8, and 10. The subcategories were and .
was evident from statements such as “I felt nothing” (1), “Because my parents had the certificate, I did not think of anything in particular” (5), and “I thought about the uses of the certificate” (10).
was expressed as, “I thought that the certificate will assist me in various ways” (3), “Because it is necessary for pensions and workers’ compensation, I undertook the procedure” (4), and “I feel that the certificate is same as a driver’s license” (8).
[Acceptance]
This category represented the state of accepting the obstacles related to the cervical spinal cord injury, and experiencing mental stability and a sense of fulfillment. It was seen in 9 out of the 10 participants, excluding Participant 10. The subcategories were , , and .
was expressed in statements such as, “I am not conscious that I am a person with cervical cord injury” (1).
was evident from statements such as, “I think the disability is a part of my personality” (2), “I was able to meet various people owing to my injury” (5), “I am alive because I had a cervical cord injury” (6), “Because I have accepted the injury and the certificate as a driver's license, I was able to go to high school” (7), “The injury is a plus in my life” (8), and “Life in the wheelchair is not too bad” (9).
was expressed in statements such as, “I do not regret that I had to ride a motorcycle” (3) and “I do not wish to restart my life again” (4).
[Lack of acceptance]
This category pertained to not being able to completely accept the obstacles related to the cervical spinal cord injury. It was seen in 7 people—Participant 1, 2, 3, 4, 6, 9, and 10. The subcategories were , , and .
was expressed in statements such as, “If I go somewhere, and there is a stair case, I return to realizing that I am a person with cervical spinal cord injury” (1) and “When I encounter something that I cannot do, I tend to think that it is because of this body” (2).
was evident from statements such as, “I don’t know which life was better” (3), “Sometimes I wish I didn’t have any injuries” (4), “I often wish that I didn’t have any injuries” (9), and “I don’t think it was good to get used to the wheelchair” (10).
was expressed as, “I want to return to being a healthy person if it is possible” (6).
[Live positively]
This category referred to the state of living life positively as a person with cervical spinal cord injury. It was seen in 8 people— Participant 2, 3, 4, 5, 6, 7, 8, and 9. The subcategories were , , , , and .
was expressed as, “I want to die laughing. I don’t want to regret it.” (2) and “I want to live as who I am” (4).
was evident from statements such as, “I want to work till I am 40 years old. I want to go for a trip after quitting work” (3), and “I want to enjoy life more” (6).
was expressed as, “I want to think positively” (5).
was expressed as, “I want to aim for the top like in the old days” (7).
was evident from statements such as, “I want to help a lot of people through basketball” (8) and “I want to help other persons with a disability” (9).
[Worry]
This category pertained to the state of worrying and feeling anxious in daily life. It was seen in all the 10 participants. The subcategories were , , and .
was expressed as, “Because I depend on my parent, I am worried about the future” (1) and “I cannot step forward if I cannot find a job” (2).
was expressed as, “I’m worried about my body” (3), “I do not know whether I can grow old like others” (4), “I’m worried about my health” (7), and “I don’t know whether I can become a parent” (8).
was evident from statements such as, “I’m worried whether I can afford to support my family” (5), “I cannot think about marriage because of my financial problems” (6), “I’m worried because I am not sure until when I can work” (9), and “I’m worried about work and marriage” (10).
Discussion
Disability acceptance process
As a result of the analysis of the disability acceptance process in each case, 23 categories were identified. Okamoto discussed that there is no uniform disability acceptance process; there are some experiences that many patients may or may not have [25]. Similarly, in our study, some categories were observed in many cases, while others were observed in all cases, showing that the disability acceptance process was not uniform and that it differed across the 10 cases.
Nine of the participants had reached the stage of subjective acceptance of disability. The categories those were common across the 10 cases were [Shock], [Effort], [Goal], [Adaptation], and [Worry]. Between the stages of [Shock] and [Effort], negative categories were observed in many cases, such as [Despair] and [Passivity]. Six cases exhibited the following order of stages: [Effort], [Goal], and [Adaptation]; while 4 cases exhibited the order [Effort], [Adaptation], and [Goal]. The subcategories of [Goal] in the former 6 cases were and , while the subcategories of the same category in the latter 4 cases were and . Honda discussed that in the activities of daily living (ADL)-independent group, patients had transitioned from physical recognition, where they gave up hope regarding recovering from the paralysis, to social recognition, where the problem was more focused on one’s social life as a person with a disability [26]. However, in the non-independent group, they remained at the level of physical recognition. The site of injury in the former 6 cases was C6, while the site of injury in the latter 4 cases was C7 and C8. Since the former cases had more severe disability than the latter did, the goals in the former cases were about their own lives, such as independence with reference to performing daily activities and returning to one’s home, while the goals in the latter cases were about social participation, such as the way of living life, ways of spending free time, and social roles, since they could perform their activities in daily life and had an idea about being at home. Finally, they reached the stage of [Worry], and regardless of whether or not they reached acceptance of disability, they worried about their future health and economic situations, such as occupation and life support.
Immediately after the injury
Immediately after the irreversible cervical cord injury due to a sudden accident, all 10 cases experienced [Shock]. In the subcategory , they were not able to understand the real situation, e.g., “I didn’t think about the inability to move” (3); “I did not understand what happened. I thought that this is how one feels when there are bruises all over the body” (6); and “I didn’t know exactly what is happening” (9). One case was optimistic without understanding the situation, as seen in the subcategory : “I expected that I would walk to home tomorrow” (8). In all 3 cases that proceeded from [Shock] to [Expecting to recover] to [Fret], the participant then moved to [Despair] and [Grief]. They had expectations that their physical function would improve immediately and that they could return to the same life as before: “I thought that I would be able to go home at the end of the month since my body did not move just because of the bruises I had all over the body” (6); “I expected that it would get better soon and that I would gradually recover” (7); “I had a positive thought that I would be able to go out with my friends again sometime” (9); however, they realized that their physical function would not fully recover: “I thought that the situation did not get better. I wondered if this would remain the same and that I would have to spend the rest of my life staring at the ceiling” (6); “I noticed that I cannot move” (7); “I started to wonder what if my body does not move” (9), and they experienced grief and were disappointed: “I was shocked since I could not to anything by myself” (7) and “I thought there is no hope in my life” (9).
Similarly, categories such as [Despair] and [Passivity] were observed after [Shock] in other cases. Studies have reported that depression was observed in some of the patients after spinal cord injury [27-29]; our results also showed that some of the participants were in a depressive condition, indicating the importance of providing psychological support, such as providing appropriate information and modifying their living environment. One report attributed the frequent occurrence of a depressive condition to the loss of hope for recovery [27]. Some of the participants became sure about their incurable condition only when they received a notification from their doctor: “My doctor told me that it would not be cured, so I thought the same” (1); “My doctor told me that I would remain bedridden, and I thought it would not be cured” (6). Thus, attention is required, in particular, after receiving a notification from doctors.
For the subcategory under the category [Despair], 3 cases were found to have suicidal thoughts: “I thought that I want to die. I despaired over life because of the injury” (5), “When I saw my disability certificate, I asked a housemaid to stab me” (6), “I wondered in what way I could die” (9). DeVivo et al. reported that 4.2-10.8% of total deaths in patients with spinal cord injury occurred due to suicide, which was the 4th to 6th highest cause of the death [30]. Furthermore, Okamoto discussed that patients with suicidal thoughts tend to feel like not doing anything, to think that their life is boring, to lose the hope to live, and to be dissatisfied with life [31]. Our results also showed that when participants had suicidal thoughts, they could possibly be depressed. Therefore, particularly careful observation is required when the participant acts passive and exhibits symptoms such as insomnia, anorexia, headache, and dizziness. Further, it is important for medical staff to be supportive and to listen to them carefully. Furthermore, it is also important to ask for help from the individual’s family if necessary.
The [Conflict] and [Repulsion] categories indicate a strong psychological conflict when the participants compared themselves with others and thought about their situation. They then felt strong anger toward themselves and others. During these phases, support from others, including medical staff, may be important. Hotta and Ichimura discussed that 1) medical staff need to attempt to always understand, in a timely manner, individual emotions and self-identity; 2) they need to understand how the patient perceives and recognizes the unconscious interactions and statements; and 3) medical care may become an opportunity for helping patients develop a positive meaning in life [21]. Sakamoto and Maeda discussed that through interactions with peers with the same disability, patients can 1) confirm that the disability is not unique to them; 2) compare themselves with others; 3) confirm their roles; 4) obtain professional knowledge and information about their future life expectations; and 5) review themselves to find themselves and make judgments regarding their disability by obtaining a reason to live and identifying new roles [32]. Okamoto reported that patients expected the medical staff to become consultation partners [33]. Therefore, medical staff is expected to act as a consultant for patients and are required to demonstrate expertise and to present roles and a reason to live. Further, special attention is required since their statements and attitudes may have an influence on the patient’s process of finding the meaning of their disability and identity.
The changing process from [Hope] and [Adaptation] and [Existence of others]
The category [Hope] indicates the condition where the participants started to have positive feelings and hope for living as persons with cervical cord injury. There were statements about , such as “I thought that I can go anywhere with a wheelchair” (5) and “I became free after I was able to get on the wheelchair” (10) showed that the transition from bed-ridden life since the cervical cord injury to free mobility with a wheelchair brought hope in the participants’ life. Furthermore, for the subcategory , there were statements such as, “Looking at a person with the same cervical spinal cord injury as mine, I thought I want to be like this person” (4), “I thought I want to put the bowl on my palm and eat the beef bowl like that person with cervical cord injury” (6). Sakamoto et al. discussed that interacting with others with the same disability fosters the understanding of the disability, and shuts down the expectations for recovery and/or negative thoughts, this influencing the process of facing life with a disability [32]. Similarly, for our participants, meeting people with the same disability due to cervical cord injury acted as an opportunity to face life with disability and move forward. Therefore, we believe that medical staff needs to establish the mobility of the patient and organize occasions to meet people with the same disability to help patients with cervical cord injury to maximally demonstrate their potential and to try new challenges with hope.
The category [Effort] indicated positive effort though statements such as, “I did my best because I hated that I could not do it because I had become disabled” (5), “I tried hard to do my own things by myself” (7), “Since I died once, I tried to make a mark before I die” (9). Oshitomi discussed that the role of medical professionals is to help the patients find a way to live with a disability [24]. Fujishiro et al. discussed that aiming for the acquisition of optimal performance of ADLs through rehabilitation leads to re-adaptation into the society and recovery of social interactions [34]. We believe that support from medical staff for the acquisition of ADL and living with the disability can lead to re-adaptation to life with the disability and to social participation.
When the process of moving from [Effort] to [Adaptation] was compared between those with an injury on C6 (hereinafter C6 group) and those with an injury on C7 and C8 (hereinafter C7 and 8 group), in the C6 group, various higher categories existed between the stages of [Effort] and [Adaptation], while only a few higher categories existed for those in the C7 and 8 groups. As discussed in the earlier section, this may be because the C7 and 8 groups may have had an earlier recovery of physical function and ADL ability as compared to the C6 group, resulting in shorter days required to be independent. Furthermore, the category [Existence of others] was observed between [Effort] and [Adaptation] in the C6 group, while it was observed between [Adaptation] and [Acceptance] in the C7 and 8 group. Again, as discussed by Sakamoto and Maeda, interacting with other people with spinal cord injury may help patients understand their injury, have realistic expectations regarding recovery, and avoid negative thoughts [32]. Indeed, this would help them face their life with a disability and would stabilize their self-concept. Ono et al. discussed that when a patient who is in serious shock receives empathy from others, the patient opens his/her mind and gains mental stability, resulting in the recovery of motivation for life [35]. In the C6 group, which had a more severe disability, other people with cervical cord injury could help the process of adaptation. On the other hand, though participants in the C7 and 8 groups may have reached adaptation without help from other people with cervical cord injury, they would need the same to reach the stage of acceptance. Furthermore, as Shinsha said, “They do not see me as a person with a disability [23]. This is only because they can accept me as a fellow, friend, and family,” it is important for medical staff to interact with patients with cervical cord injury as a person rather than as a patient.
[Acceptance] and after
The subcategories of [Acceptance], which had been achieved by 9 of the participants, were , , and . These participants expressed the following: “I am not conscious that I am a person with cervical cord injury” (1) for ; “I think the disability is a part of my personality” (2), “I am alive because I had a cervical cord injury” (6), “The injury is a plus in my life” (8), and “Life in the wheelchair is not too bad” (9) for ; and “I do not wish to restart my life again” (4) for . Hotta and Ichimura discussed that patients often developed confidence that the fundamentals of the person do not change owing to the disability [21]. Kim noted that by emphasizing on what they obtained, rather than on what they lost, patients’ confidence can be maintained or increased [4]. Similarly, we observed in the present study that the participants accepted their own disabilities, and exhibited mental stability and satisfaction. They lived positively as a person with a disability, confident in the fact that they had not changed as a person. However, one study reported that many of the patients felt hurt and/or angry when medical staff urged them to accept their disability [36], while another study reported that while a person may seem to have accepted the disability, he/she may revert to a state of intense depression [37]. Therefore, special attention is needed to avoid excessive facilitation for the acceptance of the disability from medical staff or supporters, as well as to avoid changes in the person’s mental status after acceptance.
Among the 9 participants who reached acceptance, the categories after [Acceptance] were [Lack of acceptance], [Live positively], and [Worry]. For the subcategory in [Lack of acceptance], the following comments were noted: “If I go somewhere, and there is a stair case, I return to realizing that I am a person with cervical spinal cord injury” (1), “When I encounter something that I cannot do, I tend to think that it is because of this body” (2), indicating that even after acceptance, when they encounter something that they cannot do due to their physical capacity, they return to realizing that they are persons with cervical cord injury who cannot do everything, leading them to miss what they used to have before the acceptance. Furthermore, the following statements were observed: for in [Lack of acceptance], “I don’t know which life was better” (3), “Sometimes I wish I didn’t have any injuries” (4), and “I often wish that I didn’t have any injuries” (9); for , “I want to return to being a healthy person if it is possible” (6). Hosoda reported that even after they accepted having a disability, patients tend to return to suffering like a pendulum due to trivial triggers such as failure to do something, being told about the disability by others, and good or bad weather [38]. Oshitomi discussed that even if they usually forget about their disability, they cannot help recognizing their disability in a casual situation in daily life [24]. While they live as persons with cervical cord injury, they also think about their life and family, “What if I lived as a healthy person without the injury?” and they wish to return to a healthy state if possible. This indicates that they may not have accepted the disability completely.
The category [Live positively], which indicates living positively as a person with cervical cord injury, was observed in 8 cases, except for Case 1 and another case who did not reach acceptance. The following opinions were expressed: “I want to live as who I am” (4), “I want to think positively” (5), “I want to enjoy life more” (6), “I want to aim for the top like in the old days” (7), and “I want to help other persons with a disability” (9). Hotta and Ichimura discussed that the repetitive experience of positive thinking helps the person realize what he/she can do or what his/her role is while he/she recognizes the disability, which leads to acceptance of his/her own self and life [39]. Similarly, we observed in the present study that the participants realized what they can do or what their roles were despite the restrictions in their lives due to the disability caused by the cervical cord injury. They were able to think positively, they aimed to engage in sports, hoped to help other people with a disability, and were desperate to live their lives positively.
However, all cases exhibited the category [Worry], which indicates the state of feeling anxious and worried in daily life. They expressed the following opinions: “I cannot step forward if I cannot find a job” (2), “I’m worried about my body” (3), “I’m worried whether I can afford to support my family” (5), “I cannot think about marriage because of my financial problems” (6), and “I’m worried about my health” (7), indicating that they had concerns about their own future, physical and health concerns, and financial concerns pertaining to marriage and supporting a family. The prevalence of a secondary disability in 50-year-old patients with spinal cord injury exceeds 70% [40], and the hospitalization rate due to the secondary disability has been increasing [41]. Robata pointed out that it may be due to aging [42]. Furthermore, several studies have reported that persons with disability face financial problems [43,44], indicating that, in order to live a healthy and high quality life, it is important to provide support for persons with cervical cord injury to continue living at home by preventing secondary disability and establishing financial support such as helping them seek employment that can support their life. Other studies have reported that community-dwelling persons with spinal cord injury exhibit depression even a few years after the injury [45-48], indicating the importance of provision of long-term psychological support for community-dwelling persons with spinal cord injury. Furthermore, the high necessity of care has been identified as one of the problems that persons with cervical cord injury have when they live with a family [49]. This was also expressed by one of the participants as follows: “Because I depend on my parent, I am worried about the future” (1). Presumably, this is a common problem for many persons with severe disabilities living at home. Thus, in order for persons with disability to live in the community as healthy people do, it is necessary to improve public community services and to implement policies to support persons with severe disability [50].
One person who did not reach acceptance exhibited the subcategory as a part of the category [Lack of acceptance]. Evidently, this person did not accept being a person with disability, saying, “I don’t think it was good to get used to the wheelchair” (10). Furthermore, in the category [Worry], this participant mentioned, “I’m worried about work and marriage” (10), indicating that, regardless of the acceptance, people with cervical cord injury live with concerns and worries.
Conclusion
The psychological process before and after the acceptance of disability in persons with cervical cord injury living at home involved 23 categories. Some of the categories were observed in many of the cases, while only a few categories were observed in all of the cases, indicating that the disability acceptance process was not uniform and that it involved individual differences. After the injury, we observed categories such as [Fret], [Despair], [Grief], [Passivity], [Conflict], and [Repulsion], indicating that medical staff needs to listen to patients carefully and become a familiar consultation partner who can provide professional knowledge and information, as well as help patients find a reason to live and to realize their new roles. In the process of transition from [Hope] to [Effort] and [Adaptation], medical staff needs to 1) establish mobility of the patient; 2) organize occasions for meeting other people with cervical cord injury; and 3) provide support for ADL acquisition and living with disability, during the process of acceptance of disability. In the category [Goal], persons in the C6 group had goals about their own daily activities, such as acquisition of independent ADL and returning to home because the C6 group had more severe disabilities, while persons in the C7 and 8 group had goals about their social participation, such as those pertaining to their own life, leisure activities, and social roles, since they had experienced life at home.
After [Acceptance], while they lived positively as persons with cervical cord injury, they also exhibited the category [Lack of acceptance], suggesting that they sometimes hoped to return to being a healthy person when they think about their life and family, thus returning to the thoughts that they had before the acceptance. Furthermore, worried about the future regarding their physical condition, such as health, and regarding financial concerns pertaining to marriage and family, indicating that there is a need for support for persons with cervical cord injury to continue living at home, such as 1) long-term psychological support for community-dwelling people with cervical cord injury; 2) prevention of secondary disability; 3) financial support, such as offering employment to enable them to support their life.
References
- Berger S, Garrett JF (1952) Psychological problems of the paraplegic patient. J Rehabil 18: 15-17.
- Frank RG, Van Valin PH, Elliott TR (1987) Adjustment to spinal cord injury - A review of empirical and nonempirical studies. J Rehabil 53: 43-48.
- Elliott TR, Frank RG (1996) Depression following spinal cord injury. Arch Phys Med Rehabil 77: 816-823.
- Kim R (1997) The Psychological problems and adaptation of persons with spinal cord injuries: A prospect from rehabilitation psychology. Bulletin of the Graduate School of Education, the University of Tokyo 37: 177-183.
- Bulman RJ, Wortman CB (1977) Attributions of blame and coping in the “real world”: Severe accident victims react to their lot. J PersSocPsychol 35: 351-363.
- Grayson M (1951) Concept of “acceptance” in physical rehabilitation. J Am Med Assoc 145: 893-896.
- Dembo T, Leviton GL, Wright BA (1956) Adjustment to misfortune: A problem of social-psychological rehabilitation. Artificial Limbs 3: 4-62.
- Wright BA (1960) Physical disability: A psychological approach. New York: Harper & Brothers Publishers.
- Cohn N (1961) Understanding the process of adjustment to disability. J Rehabil 27: 16-18.
- Fink SL (1967) Crisis and motivation: A theoretical model. Arch Phys Med Rehabil 48: 592-597.
- Siller J (1969) Psychological situation of the disabled with spinal cord injuries. Rehabil Lit 30: 290-296.
- Tucker SJ (1980) The psychology of spinal cord injury: Patient-staff interaction. Rehabil Lit 41: 114-121.
- Weller DJ, Miller PM (1977) Emotional reactions of patient, family, and staff in acute-care period of spinal cord injury: Part 1. Soc Work Health Care 2: 369-377.
- Ueda S (1980) Acceptance of disability. Gen Rehabil 8: 515-521.
- Furumaki S (1977) Process of adjustment to physically disability. Japanese J PhysTherOccupTher 11: 721-726.
- Kendall E, Buys N (1998) An integrated model of psychosocial adjustment following acquired disability. J Rehabil 64: 16-20.
- Parker M, Schaller J, Hansmann S (2003) Catastrophe, chaos, and complexity model and psychosocial adjustment to disability. RehabilCouns Bull 46: 234-241.
- Bishop M (2005) Quality of life and psychosocial adaptation to chronic illness and acquired disability: A conceptual and theoretical synthesis. RehabilCouns Bull 48: 219-231.
- Shontz FC (2003) Rehabilitation psychology, then and now. RehabilCouns Bull 46: 176-181.
- Nagumo N (2003) Acceptance of disability and social interactions-social acceptance as an effective method of self-acceptance. Gen Rehabil 31: 811-814.
- Hotta R, Ichimura K (2009) Research on acceptance of disability in individuals with spinal cord injury. Ibaraki Prefectural University of Health Sciences 26: 31-39.
- Nakajima S, Inoue K (2005) Acceptance of disability that through a spinal cord injury patient’s physical therapy. J PhysTherPrac Res 14: 23-26.
- Shinsha N (2003) Can disabled persons accept their disabilities? Gen Rehabil 31: 815-820.
- Oshitomi T (2013) Acceptance of disability. Japanese J OccupTher 47: 1354-1358.
- Okamoto I (2003) Acceptance of disability and tendencies towards suicidal thoughts in stroke patients. The Japanese Journal of Rehabilitation Medicine 40: 531-536.
- Honda T (1988) Relationship between the process of awareness of disability and rehabilitation programs in patients with spinal cord injuries. The Japanese Journal of Rehabilitation Medicine 25: 43-55.
- Fullerton DT, Harvey RF, Klein MH, Howell T (1981) Psychiatric disorders in patients with spinal cord injuries. Arch Gen Psychiatry 38: 1369-1371.
- Howell T, Fullerton DT, Harvey RF, Klein M (1981) Depression in spinal cord injured patients. Paraplegia 19: 284-288.
- Judd FK, Stone J, Webber JE, Brown DJ, Burrows GD (1989) Depression following spinal cord injury: A prospective in-patient study. Br J Psychiatry 154: 668-671.
- DeVivo MJ, Black KJ, Richards JS, Stover SL (1991) Suicide following spinal cord injury. Paraplegia 29: 620-627.
- Okamoto I (2014) Support of mind in stroke patients, agony, discouragement, tendencies towards suicidal thoughts and acceptance of disability. Modern Physician 34: 793-796.
- Sakamoto M, Maeda T (2002) Factors influencing mental recovery from distress in patients with spinal injury. Journal of Japan Society of Nursing Research 35: 439-449.
- Okamoto I (2013) Acceptance of disability: The mindset of stroke patients. The Japanese Journal of Rehabilitation Medicine 50: 951-956.
- Fujishiro Y, Hasegawa T, Hirabe M, Ihara K, Takayanagi M, et al. (2001) Social participation of people with traumatic spinal cord injury. Gen Rehabil 29: 151-159.
- Ono M, Takayama T, Kusano E, Kawata C (2007) Peer support patients and its relationship with mental health-survey on the ostomates. Japan Journal of Nursing Science 27: 23-32.
- Hosoda M (2006) Meaning to live in a stroke; Sociology of illness and disability. Tokyo: Seikaisya.
- Aouda T (2008) From the situation of the nurse, acceptance of disability and state of the care to show in a nursing care. Rehabil Nurse 1: 590-594.
- Hosoda M (2009)Acceptance of disability’ revisited. Gen Rehabil 37: 899-902.
- Hotta R, Ichimura K (2011) Nurses perception of acceptance of disability with the convalescent spinal cord injury patients. Journal of Japan Society of Nursing Research 34: 21-30.
- Kumakura N, Takayanagi M, Hasegawa T, Ihara K, Yano H, et al. (2002) Self-assessed secondary difficulties among paralytic poliomyelitis and spinal cord injury survivors in Japan. Arch Phys Med Rehabil 83: 1245-1251.
- Cardenas DD, Hoffman JM, Kirshblum S, McKinley W (2004) Etiology and incidence of rehospitalization after traumatic spinal cord injury: A multicenter analysis. Arch Phys Med Rehabil 85: 1757-1763.
- Robata BT (1986) Aging with a disability. New York: Demos Medical Publications.
- Kajiwara T, Takahashi K (1994) Acceptance of physical disability in patients with stroke. Gen Rehabil 22: 825-831.
- Kawamura J, Ikeyama H, Ibata E (1994) What is required in quadriplegic patients for living at home? Journal of Clinical Rehabilitation 3: 568-573.
- Fuhrer MJ, Rintala DH, Hart KA, Clearman R, Young ME (1993) Depressive symptomatology in persons with spinal cord injury who reside in the community. Arch Phys Med Rehabil 74: 255-260.
- MacDonald MR, Nielson WR, Cameron MG (1987) Depression and activity patterns of spinal cord injured persons living in the community. Arch Phys Med Rehabil 68: 339-343.
- Nagumo N, Yamada R, Takayama T, Chida T, Matsuura M (1989) Survey on psychological adjustments following spinal cord injury and brain injury. Res Bull Nat Rehabil Cent Disabled 10: 75-108.
- Schulz R, Decker S (1985) Long-term adjustment to physical disability: The role of social support, perceived control, and self-blame. J PersSocPsychol 48: 1162-1172.
- Hasegawa Y, Ando N, Hayashi T, Okawa T (1990) Social problem of the aged spinal cord injury patients. Gen Rehabil 18: 439-443.
- Matsui K (1988) About target of coming back to life of persons of high rank among cervical spinal cord patients. J Japan Med Soc Paraplegia 1: 110-111.