Management of Vestibular Schwannoma
At the beginning of the 20th century patients with VS suffered a non-choice between an agonizing death and attempted surgical excision. Early operations carried with an unacceptable risk of mortality. At the 1913 International Conference of Medicine in London the three foremost surgeons of the time (Horsley, Eiselberg and Krause) reported a greater than 50% mortality rates from small patient cohorts. Those who survived surgery inevitably suffered significant disability.
Throughout the century advances in surgical technique reduced operative mortality to less than 1%. By the turn of the millennium the natural history of the condition was well understood, and novel treatment techniques such as gamma knife were competing with surgery to improve patient care. This review examines the current management of VSs, and establishes trends that will continue as the century progresses.
Imaging is focal to the modern management of vs. Magnetic Resonance Imaging (MRI) scanners allow accurate depiction of tumor size and location. These advances have brought an increased understanding of the natural history of vs. An observational study conducted between 1975 and 2005, showed that of 729 VS patients who had serial MRI scans performed only a small percentage showed active growth (17% of intrameatal and 29% of extrameatal). Furthermore, age and gender were not predictive of tumor growth [1].
Such studies have made ‘observation’ a viable management option, as it is now understood that it is not justified to operate on a minimally symptomatic static tumor. A ‘watch and wait’ approach is utilized for ‘small’ tumors. A recent meta-analysis has helped to define the present role of conservative management. It included 21 studies totaling 1,345 patients. The mean initial tumor size was 11.8 mm, 43% showed slow growth, and 57% showed no growth or tumor regression. Hearing loss was observed in 51% of those tested [2].
Stereotactic radiosurgery, or ‘gamma knife’, involves fixing a frame to the patient’s head and delivering a high dose of targeted radiation to a pathological lesion. It differs from orthodox radiotherapy in that only a single dose of radiation is required, rather than a functional course. The dramatic treatment outcomes possible using the technology became apparent from an early stage. A study of 256 acoustic neuromas treated with gamma knife therapy between 1969 and 1991 showed early loss of contrast enhancement in 70%, with a reduction in the unilateral tumor size in 55%, with only 12% increasing in size [3].
The technique can provide equivalent results to surgery, without any of the accompanying risks, of infection, bleeding or CSF leak, and requires no period of hospitalization. Furthermore there is no possibility of tumor seeding, which has been documented years after the surgical excision of the primary lesions [4].
The technology is continually improving and becoming more precise, as this process occurs the effective radiation dose is being reduced. Most centres use 12-13 Gy to the margin of the tumor. This protocol carries with it a 1% risk of facial nerve palsy, with similar rates observed for trigeminal neuropathy. The risks of iatrogenic injury are likely to fall further.
Whilst its exact role has been a source of some contention, it is now accepted to provide an alternative to surgery for tumors of less than 3 cm, in their maximum diameter [5].
The setup is shown diagrammatically below
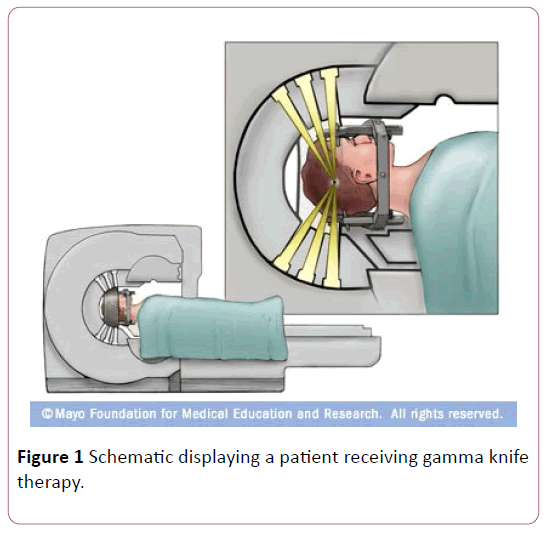
Figure 1 Schematic displaying a patient receiving gamma knife therapy.
The impact of the technology has been profound. Analysis of the 1998 and 2008 patient surveys from the acoustic neuroma association of the USA, showed that radiosurgery and watch and wait were growing in popularity (Patel et al., 2014). Similarly a retrospective analyses of the US national inpatient sample database from 2000-2007 showed that there was a 41% reduction in surgical excision of vs. Over the same period there was a rise in the non-routine discharge and complication rates. The authors speculate that this may have occurred as the remaining surgery takes place on larger, more complex tumors [6].
In the United Kingdom data from the Oxford skull base clinic has shown a movement away from surgery and towards gamma knife. The authors recognize the role surgery plays will be increasingly confined to ‘giant’ tumors [7].
The technique does have some weaknesses. Patients need to be followed up over a longer period than for surgical management. Secondly, there is a risk of the radiation dose causing malignant transformation. A recent study attempted quantification and found that without radiation the risk of malignancy is 1.32-2.08 per 100,000, although this is inflated by the inclusion of Neurofibromatosis 2 cases. Following radiation treatment the overall risk of malignancy rises to 25 per 100,000. This implies a greater than 10 fold increase in risk is malignancy following gamma knife therapy [8]. Furthermore, there is concern that the radiation dose can cause scarring, which makes any subsequent surgery more difficult.
The third and still predominant treatment modality for VS is surgery. In the UK the VS surgery is performed by a select group of 28 neurologists, 22 of whom work directly with neurosurgical assistants. Three surgical approaches are recognized, retrosigmoid, translabyrinthine and middle cranial fossa. There is little agreement on exactly when to utilize each approach with 7/28 using tumor size to dictate the approach, whilst 8 exclusively utilize the sub occipital or retrosigmoid approach, and 10 exclusively the translabyrinthine [9].
The approaches are shown in the schematic below
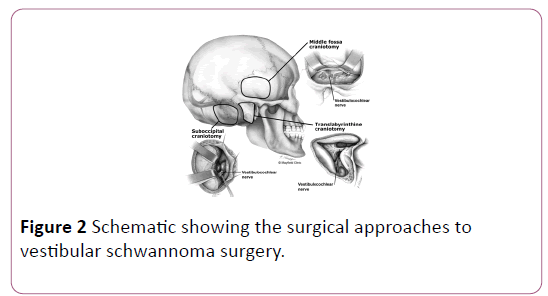
Figure 2: Schematic showing the surgical approaches to vestibular schwannoma surgery.
The translabyrinthine approach is preferred by the majority of neurotologists. Some of its detractors have suggested that it only provides minimal access to the posterior fossa, however, in skilled hands this criticism is unfounded, and any size of tumor can be removed. Further, the technique allows early identification of the facial nerve is possible, facilitating potential repair if required. As the name implies the approach goes directly through the labyrinth, so any residual hearing is destroyed.
The middle cranial fossa approach is decreasing in popularity as it provides only cramped access to the cerebellopontine angle, and requires temporal lobe retraction, which carries with it the risk of post-operative seizures.
The retrosigmoid approach evolved from the classic suboccipital operations originally performed for aneurysms. There is no limit to the size of tumor which can be removed through such an approach, and any residual hearing can be preserved. The only disadvantages are the poor view of fundus, and there is an increased risk of postoperative headache. A recent study showed the cost of resecting a vestibular neuroma was significantly less for translabyrinthine than retrosigmoid approaches [10]. The reasons for this were multifactorial but was mainly explained by the increased length of hospital stay and ICU admission associated with the retrosigmoid approach.
All of the principles of management discussed relate to both unilateral sporadic tumors as well as bilateral tumors caused by underlying syndromes. Neurofibromatosis type 2 (NF2) is a tumor predisposition syndrome, caused by a dominant mutation on chromosome 22. Sufferers classically develop bilateral vs. as early as the third decade. The management of such cases has some specific nuisances [11]. Firstly, long term follow up has shown that gamma knife is less effective in cases of neurofibromatosis than unilateral cases [12]. Consequently, the rate of surgical management is declining at a slower rate in NF2 cases [13]. As tumors are often bilateral patients have no VIII th nerves following surgery, meaning rehabilitation often takes the form of Auditory Brainstem Implants which bypass the missing nerves to give some functional hearing.
It is well acknowledged that there is a shortage of high quality comparative evidence; this has made the creation of accurate guidelines problematic. The literature is full of partisan claims but few have followed a definitively evidenced based approach. An English language medical literature search has been conducted over the past 23 years dealing with outcomes following vs. treatment. 111 studies were included of which 95 reported type 3 evidence and 6 reported type 4 evidence. None of the studies included were supported by type 1 or type 2 evidence [14]. There is at present no high quality evidence within the literature from randomized control trials to compare stereotactic radiotherapy with microsurgical resection or observation alone [15]. Whilst this remains the case the treatment method chosen will be highly subjective. Such choices are likely to show great variability between different centres and surgeons. Presently, the decision is based on a number of patient, tumor and surgeons factors.
One clear area for comparison is the propensity of treatment to treat or exacerbate the otological symptoms of VS. The most bothersome symptom to many patients is tinnitus. Recent studies have suggested that post treatment levels of tinnitus do not differ across the different treatment modalities of open microsurgery, radiosurgery, and observation [16]. Further work, has shown even when the cochlear nerve is cut intraoperatively tinnitus remains unchanged in 37% of cases [17]. It is suggested that in these cases the tinnitus has become established in brainstem or post brainstem pathways at the time of surgery. It is therefore not appropriate to guide management decisions based upon the likely impact on the patient’s tinnitus.
Other studies have looked at the impact on mental health measures of depression and anxiety induced by different managements. A cross sectional questionnaire was completed by 205 adults who were pre or post treatment for unilateral acoustic neuroma. The results showed that mean anxiety and depression scores did not differ from the general population, and were not different across separate treatment modalities [18].
Similarly, attempts have been to look at quality of life indices for different treatment modalities. A recent study looked at responses to the Penn Acoustic Neuroma Quality of Life (PANQOL). The PANQOL general wellbeing scores were found to be significantly lower in the conservatively managed group. However, the authors concede that the conclusions that could be drawn from the work are limited by demographic differences in age and associated comorbidities [19-26]. A truly randomized study would be unethical.
To conclude, 21st century management of VS encompasses a multidisciplinary team approach to the patient care. As imaging techniques and gamma knife have improved there has been a clear movement away from surgery. This is almost certain to continue. As the number of operations falls the service is likely to become increasingly centralized, with a core of specialist neurotologists performing increasingly bespoke operations. A clear target for the first half of the 21st century is to improve the evidence base to produce clear guidelines for such cases. The nature of VS management in the second half of the century is in the realms of speculation. However the possibility of an eventual pharmalogical cure is not impossible. Such a development will mean that the all morbidity associated with current treatment paths such as iatrogenic facial nerve palsy can be consigned to history. 21st century otolaryngologists can be relieved that unilateral tinnitus or hearing loss no longer includes a differential diagnosis, which one hundred years ago represented a death sentence.
‘She was aged 26 years, complete blindness, incomplete deafness, numbness of the skin of the face, unbearable headaches, continual nausea, violent efforts at vomiting, convulsive contractions of the facial muscles.
She expressed a passionate wish to die as the sole means of ending her suffering. After a state of unusually prolonged calm the patient lost consciousness and died after an agonising 24 hours.
References
- Stangerup SE, Thomasen PC, Tos M, Thomsen J (2006). The natural history of vestibular schwannoma. OtolNeurotol 27: 547-552.
- Smouha EE, Yoo M, Mohr K, Davis RP (2005) Conservative Management of Acoustic Neuroma: A Metaâ€ÂÂÂÂAnalysis and Proposed Treatment Algorithm. Laryngoscope 115: 450-454.
- Norén G, Greitz D, Hirsch A, Lax I (1993) Gamma knife surgery in acoustic tumors. In Advances in Stereotactic and Functional Neurosurgery 10: 104-107.
- Roser F, EbnerFH, Skardelly M (2016) The possibility of seeding vestibular schwannomas through surgery: Limited experience with two cases. SurgNeurolInt 7: S291-S294.
- Rowe JG, Radatz MWR, Walton L, Hampshire A, Seaman S, et al. (2003) Gamma knife stereotactic radiosurgery for unilateral acoustic neuromas. J NeurolNeurosurg Psychiatry 74: 1536-1542.
- Patel S, Nuño M, Mukherjee D, Nosova K, Lad SP et al. (2013) Trends in surgical use and associated patient outcomes in the treatment of acoustic neuroma. World Neurosurg 80: 142-147.
- MacKeith SA, Kerr RS, Milford CA (2013) Trends in acoustic neuroma management: a 20-year review of the oxford skull base clinic. J NeurolSurg B Skull Base 74: 194.
- SeferisC, Torrens M, Paraskevopoulou C, Psichidis G (2014) Malignant transformation in vestibular schwannoma: report of a single case, literature search, and debate: Case Report. Lancet 121: 160-166.
- Saeed SR, Suryanarayanan R, Dezso A, Ramsden RT (2006) Vestibular schwannoma management: current practice amongst UK otolaryngologists–time for a national prospective audit. The Annals of The Royal College of Surgeons of England 88: 490-495.
- Semaan MT, Wick CC, Kinder KJ, Stuyt JG, Chota RL, et al. (2015) Retrosigmoid versus translabyrinthine approach to acoustic neuroma resection: A comparative costâ€ÂÂÂÂeffectiveness analysis. Laryngoscope 126: S5-S12.
- Evans DGR, Lloyd SKW, Ramsden RT (2011) Neurofibromatosis type 2.Medical Genetics in the Clinical Practice of ORL 70: 91-98.
- Sun S, Liu A (2014) Long-term follow-up studies of Gamma Knife surgery for patients with neurofibromatosis Type 2: Clinical article J Neurosurg121: 143-149.
- Mahboubi H, Maducdoc MM, Yau AY, Ziai K, Ghavami Y, et al. (2015) Vestibular Schwannoma Excision in Sporadic versus Neurofibromatosis Type 2 Populations. Otolaryngol Head Neck Surg 153: 822-831.
- Nikolopoulos TP, O'Donoghue GM (2002) Acoustic neuroma management: an evidence-based medicine approach. OtolNeurotol 23: 534-541.
- Muzevic, D,Legcevic J, Splavski B, Cayé-Thomasen P (2014) Stereotactic radiotherapy for vestibular schwannoma. Cochrane Database of Systematic Reviews.
- Overdevest JB, Pross SE, Cheung SW (2015) Tinnitus following treatment for sporadic Acoustic neuroma. The Laryngoscope 126: 1639-1643.
- Kohno M, Shinogami M, Yoneyama H, Nagata O, Sora S, et al. (2014) Prognosis of tinnitus after acoustic neuroma surgery—surgical management of postoperative tinnitus. World Neurosurg 81: 357-367.
- Brooker JE, Fletcher JM, Dally MJ, Briggs RJS, Cousins VC, et al. (2012) Factors associated with anxiety and depression in the management of acoustic neuroma patients. J ClinNeurosci 19: 246-251.
- McLaughlin EJ, Bigelow DC, Lee MY, Ruckenstein MJ (2013) Quality-of-Life Differences by Treatment Groups for Acoustic Neuroma Patients. J NeurolSurg B Skull Base 74: A126.
- Fan YW, Yu CP, LeungKM (2014) Towards zero facial palsy in management of large acoustic neuroma: combining the merits of microsurgery and radiosurgery. Hong Kong Neurosurgical Society.
- Gleeson MJ, Clarke RC, editors (2008) Scott-Brown's Otorhinolaryngology: Head and Neck Surgery, 7Edn, volume3, CRC Press.
- Lam R (2015) Acoustic neuroma manifesting as toothache and numbness.Aust Dent J.
- Lee SH, Choi SK, Lim YJ, Chung HY, Yeo JH, et al. (2015) Otologic manifestations of acoustic neuroma. ActaOtolaryngol135: 140-146.
- Malik TH, Kelly G, Ahmed A, Saeed SR, Ramsden RT (2005) A comparison of surgical techniques used in dynamic reanimation of the paralyzed face. OtolNeurotol26: 284-291.
- Patel J, Vasan R, van Loveren H, Downes K, Agazzi S (2014) The changing face of acoustic neuroma management in the USA: analysis of the 1998 and 2008 patient surveys from the acoustic neuroma association. Br J Neurosurg 28: 20-24.
- Silva J, Cerejo A, Duarte F, Silveira F, Vaz R (2012) Surgical removal of giant acoustic neuromas. World Neurosurg 77: 731-735.