Keywords
HCC; Doxorubicin; Rosuvastatin; Captopril; Omega-3
Introduction
Hepatocellular carcinoma (HCC) is the third most common cause of cancer-related death and the leading cause of death in Europe and in the US [1,2]. The Most causes of HCC mediate liver injury through the development of liver inflammation and fibrosis, which leads to the disordered liver architecture characteristic of liver cirrhosis [3,4]. Resistance of HCC cells to apoptosis is a crucial aspect in cancer treatment because it impairs the efficacy of different therapy regimens [5]. In addition, HCC is one of the most vascular tumors and is characterized by an abnormal vascular structure. Hepatocarcinogesis is characterized by high level of vascular endothelial growth factor (VEGF) and platelet derived growth factor (PDGF). Therefore, the interesting targets for anticancer therapies are VEGF and its receptors [6].
Doxorubicin (DOX) is considered one of the most effective drugs in the treatment of lymphomas, breast adenocarcinomas, liver cancer and other malignant tumors [7,8]. However, like most of the anticancer drugs, DOX causes various toxicity effects, the commonest of which is dosedependent cardiotoxicity. The primary mechanism of DOXinduced cardiotoxicity (DIC) is due to generation of reactive oxygen species (ROS), clinical approaches designed to attenuate the DOX-induced cardiotoxicity consist of antioxidation, iron chelation, and free radical scavenging but the results were disappointing [9-11].
Statins have been suggested to decrease the risk of some cancers, although available data are conflicting [12,13]. Statins have been shown to arrest tumor and normal cells in the G1 phase of the cell cycle, inducing a potent apoptotic effect [14]. Statins are also known to decrease free radical generation in the vascular wall and in the myocardium during ischemia reperfusion injury [12]. Rosuvastatin (ROV), a specific competitive inhibitor of the enzyme 3-hydroxyl-3- methylglutaryl coenzyme A (HMG-CoA) reductase [14] is one of the potent and relatively new statins.
Omega-3 is poly unsaturated fatty acids has been shown to reduce the size of tumors and enhance the positive effects of chemotherapeutic drugs , reducing systemic inflammation, and oxidative stress – all processes that have been linked with tumor growth [15]. Omega- 3 has potent anti-angiogenic effect, inhibiting production of many important angiogenic mediators including VEGF and PDGF [16].
Angiotensin converting enzyme inhibitors (ACE-Is) are widely used as antihypertensive agents and have been suggested to decrease the intra-tumoral blood flow without affecting healthy organs [17]. Additionally, the antioxidant enzymes and non-enzymatic antioxidant defenses are increased due to captopril treatment in different mouse tissues [18].
The aforementioned information prompted us to study the possibility of a combined therapeutic intervention using rosuvatatin, captopril or omega 3 with lower doses of DOX. This therapeutic scheme would likely decrease the cardiotoxic effects of DOX, while improving the efficacy of the therapeutic response.
Materials and Methods
Animals
The present work was carried out on 48 male Albino mice, 6-8 weeks old weighing 20 ± 5 gm. Mice were housed in stainless-steel mesh cages (n=8) under standard conditions of light illumination (light/dark 12 h/12 h cycle), temperature (22 ± 3°C), and humidity (60 ± 10%). Animals were allowed access to food and tap water ad libitum throughout the acclimatization and experimental periods. The study was conducted according to the international guidelines and approved by the Ethics Committee for Animal Experimentation of Faculty of Pharmacy, Cairo University (Permit number: PT 1323).
Chemicals
Diethylnitrosamine (DEN) was purchased from (Sigma Chemical Co. St. Louis, USA) Doxorubicin (DOX) 10 mg/vial, Captopril (CAP) 25mg/tablet, Rosuvastatin (ROV) 10mg/tablet and Omega 3 (OMEGA) 1000mg/capsule were supplied by ( Pfizer, USA) (Galxosmithklline, UK) (Astrazenca, UK) and (Sedico, Egypt ) respectively. All other chemicals and reagents were purchased from Chematech Co (Alexandria, Egypt).
Experimental design
Induction of hepatocellular carcinoma: Hepatocellular carcinoma (HCC) was induced in male mice by weekly intraperitoneal injection of DEN in a dose of 75 mg/kg body weight for 3 weeks, followed by 100 mg/kg body weight weekly for the next 3 weeks [19].
Experimental protocol
Mice were randomly divided into six groups (n=eight in each group):
Group-I negative control group: Mice in this group received phosphate-buffered saline (PBS) in weekly to serve as normal controls for the other treated groups.
Group-II positive control group (DEN group): Mice in this group received only the carcinogenic agent DEN ip for six weeks as previously mentioned. At the end of 8th week after DEN administration, following confirmation of incidence of HCC, mice was randomly assigned to one of the following subgroups for treatment:
Group-II (a): DOX – treated group (DOX group): Mice in this group were treated with DOX (12 mg/kg b.wt, ip) 3 mg/kg every other day for four consecutive doses starting from the 9th week [20].
Group-II (b): (DOX +ROV) – treated group (ROV group): Mice in this group were treated with DOX (similar to group-II (a)) and with a daily oral dose of rosuvastatin (20 mg/kg b.wt.) via an oral gavage syringe [21].
Group-II (c): (DOX + Omega-3) – treated group (OMEGA group): Mice in this group were treated with DOX (similar to group-II (a)) and with a daily oral dose of omega 3 (1 gm /kg b.wt.) [22].
Group-II (d): (DOX+CAP) – treated group (CAP group): Mice in this group were treated with DOX (similar to group II-a) and with a daily oral dose of captopril (25 mg /kg b.wt.) [23]. All treatment regimens were given for 21 days starting from the 9th week. The design of treatment is shown in Figure 1
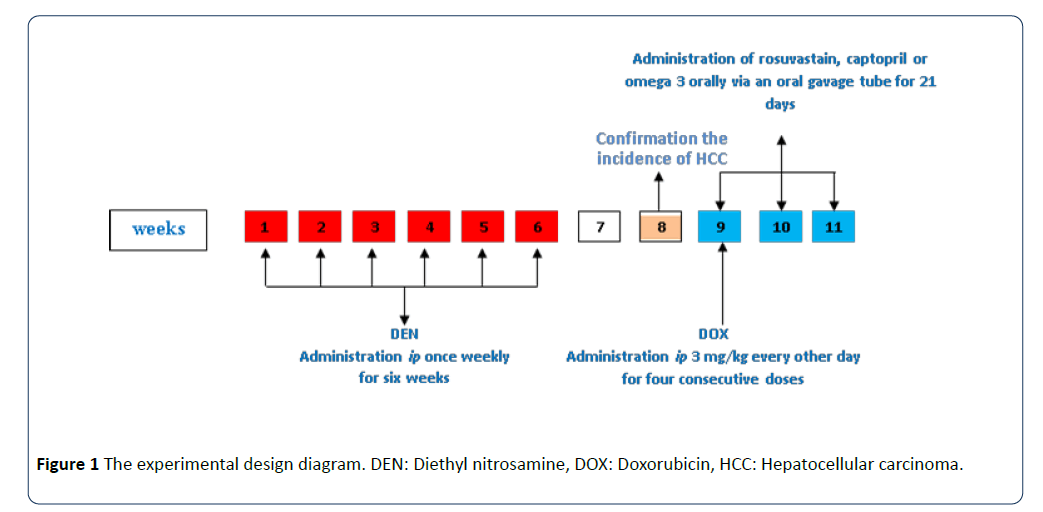
Figure 1: The experimental design diagram. DEN: Diethyl nitrosamine, DOX: Doxorubicin, HCC: Hepatocellular carcinoma.
At the end of the treatment period, animals were sacrificed by cervical dislocation. Tumor liver tissues and hearts were removed, immediately chilled on ice and weighed. Each excised liver and heart was divided into several parts for further assessment. Noticeably, some assessments were carried out immediately after excision. The remaining portions of liver and heart specimens were snap-frozen and kept at - 80°C till used.
The following parameters were determined:
Histopathological examination [24]: Formalin-fixed, paraffin-embedded 3 to 4 μm liver and heart tissue sections were prepared and stained routinely by H&E for histopathologic examination. Tumor grade was scored using the modified nuclear grading scheme outlined by Edmondson and Steiner, [25] with tumor grade categorized as well, moderately and poorly differentiated.
Determination of angiogenic parameter in crude liver tissue extracts: Determination of vascular endothelial growth factor (VEGF) in liver tissue homogenate was measured with a mouse ELISA kit (eBiosciences Inc., SanDiego, CA92121,USA) in accordance with the supplier's instructions (Mathonnet et al., 2006) [26].
Determination of tumor cell viability using the trypan blue exclusion test [27]: After the end of treatment period, primary tumors were collected and cells were filtered through a 40-lm cell strainer (Fisher, Hampton, NH, Cat no. 22363547) to obtain single-cell suspensions. The number of viable cells present in a cell suspension is determined by dye exclusion test. It is based on the principle that live cells possess intact cell membranes that exclude certain dyes, such as trypan blue, Eosin, or propidium, whereas dead cells do not.
Immunohistochemical determination of pro-and antiapoptotic molecules Bak and Bcl-x in liver tissues: Further liver sections on coated slides were performed for immunohistochemical staining using avidin biotin peroxidase complex method [28]. Briefly, after inhibition of endogenous peroxidases with 3% hydrogen peroxide, slides were treated with microwave in 10 mm citrate buffer for 15 minutes. After washing the slides in tris buffered saline (TBS), they were incubated with 10% normal goat serum at 23°C for 30 minutes. Slides were then incubated at 4°C overnight with the following primary antibodies: 200 μg/ml prediluted rabbit Bak monoclonal antibody. (Cat. #RB-1520, Thermo Fisher Scientific Fremont, CA 94538, USA) or 200 μg/ml Prediluted mouse Bcl-X monoclonal antibody (Cat. #MS-715, Thermo Fisher Scientific Fremont, CA 94538, USA).
Evaluation of Bak or Bcl-X [29]: Expression of Bak or Bcl-X in selected microscopic fields (×400) was semi-quantitatively evaluated on the basis of the percentage of positive cells and classified as follows: when positive cells accounted for less than 10% of total cells; negative staining (-), 10–25%; weak staining (+), 26–50%; moderate staining (++) and > 51%; strong staining (+++).
Determination of inflammatory parameter (TNF – α) and oxidative stress parameters (MDA, GSH, SOD) in crude heart tissue extracts: Tumor necrosis factor- α (TNF- α) was assayed in crude heart extracts. This was done by ELISA using kit commercially avaliable from eBioscience® Inc., Cat. # RMTNFAI, San Diego, USA [30]. Additionally, thiobarbituric acid (TBA) test procedure described by Uchiyama and Mihara (1978) [31] is the most frequently used index of lipid peroxidation in various animal tissue homogenates. The TBA is frequently referred to MDA (Malondialdehyde), which is generated by autoxidation of the polyunsaturated fatty acids PUFAs or esters containing three or more double bonds [32]. Furthermore, the glutathione in reduced form (GSH) was measured according to Murphy’s method [33]. Moreover, the activity of superoxide dismutase (SOD) was determined by pyrogallol method of Marklund and Marklund [34].
Statistical analysis: Quantitative data were described using median as well as mean ± SD. Comparisons between groups were performed with the nonparametric Mann–Whitney test in the case of abnormally distributed continuous variables. Significance of the obtained results was judged at the 5% level.
Result
Conventional pathological assessment of mouse liver by Haematoxylin and Eosin (H&E) staining:
Histopathological studies of H&E stained sections of hepatic tissue specimens revealed that mice treated with DEN had developed either a well or moderately differentiated HCC. They showed large irregular nuclei with coarse chromatin and prominent nucleoli, pleomorphic large irregular nuclei with prominent nucleoli and pseudoinclusion with no to low apoptotic cells. Treatment with doxorubicin also caused no significant apoptosis. In contrast, addition of rosuvasatin, captopril or omega3 to doxorubicin causes a significant apoptosis more than doxorubicin alone. However, ROV or CAP groups produced more significant apoptosis than OMEGA group. Figure 2 illustrates the different histopathological changes detected in the different experimental groups.
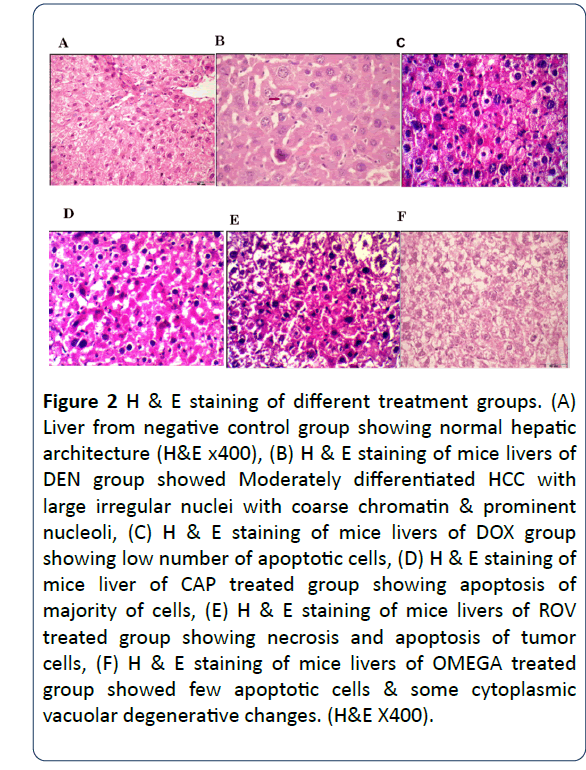
Figure 2: H & E staining of different treatment groups. (A) Liver from negative control group showing normal hepatic architecture (H&E x400), (B) H & E staining of mice livers of DEN group showed Moderately differentiated HCC with large irregular nuclei with coarse chromatin & prominent nucleoli, (C) H & E staining of mice livers of DOX group showing low number of apoptotic cells, (D) H & E staining of mice liver of CAP treated group showing apoptosis of majority of cells, (E) H & E staining of mice livers of ROV treated group showing necrosis and apoptosis of tumor cells, (F) H & E staining of mice livers of OMEGA treated group showed few apoptotic cells & some cytoplasmic vacuolar degenerative changes. (H&E X400).
Effect of different treatment regimens on the level of VEGF (pg/ml) in mouse liver:
The effect of different treatment regimens on the level (pg/ml) of VEGF in mice livers is shown in Figure 3. The highest concentration of hepatic VEGF level (3914 ± 186 pg/ml) was found in the DEN group compared to the negative control group. Compared to the DEN group, administration of doxorubicin (12 mg/kg ip) resulted in a significant decrease of hepatic VEGF level (3532 ± 144 pg/ml). However, higher decrease was observed in CAP, ROV and OMEGA treated groups.
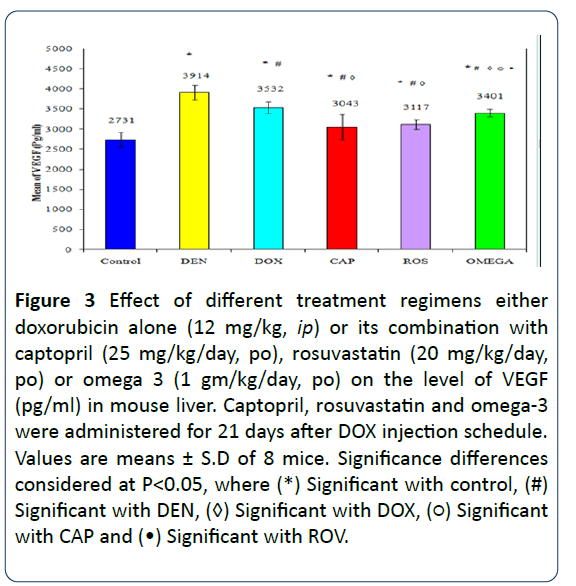
Figure 3: Effect of different treatment regimens either doxorubicin alone (12 mg/kg, ip) or its combination with captopril (25 mg/kg/day, po), rosuvastatin (20 mg/kg/day, po) or omega 3 (1 gm/kg/day, po) on the level of VEGF (pg/ml) in mouse liver. Captopril, rosuvastatin and omega-3 were administered for 21 days after DOX injection schedule. Values are means ± S.D of 8 mice. Significance differences considered at P?0.05, where (*) Significant with control, (#) Significant with DEN, (◊) Significant with DOX, (?) Significant with CAP and (•) Significant with ROV.
Effect of different treatment regimens on the percentage of tumor cell viability in HCC:
The percentage of tumor cell viability in livers of the different groups is expressed in Figure 4. The percentage of tumor cell viability in mice livers treated only with DEN ranged from (95-99%). It was decreased significantly in livers of DOX treated group compared to DEN treated group. On the other hand, CAP, ROV and OMEGA-treated groups showed a significant decrease in comparison with the DOX group.
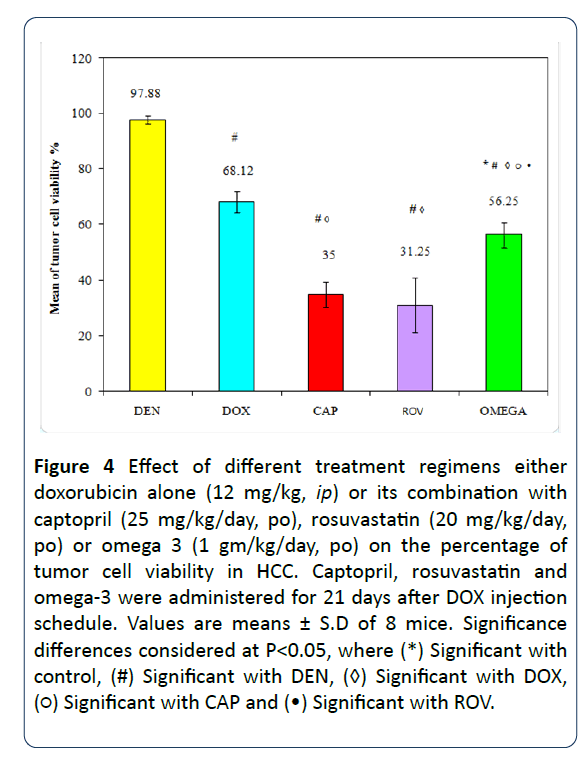
Figure 4: Effect of different treatment regimens either doxorubicin alone (12 mg/kg, ip) or its combination with captopril (25 mg/kg/day, po), rosuvastatin (20 mg/kg/day, po) or omega 3 (1 gm/kg/day, po) on the percentage of tumor cell viability in HCC. Captopril, rosuvastatin and omega-3 were administered for 21 days after DOX injection schedule. Values are means ± S.D of 8 mice. Significance differences considered at P?0.05, where (*) Significant with control, (#) Significant with DEN, (◊) Significant with DOX, (?) Significant with CAP and (•) Significant with ROV.
Effect of different treatments on expression of Bak and Bclx (proapoptotic and antiapoptotic protein) immunohistochemically in tumor tissue sections:
Bak expression was zero in DEN-treated group (Figures 5). However, intensity of Bak expression increased significantly in mice livers treated with rosuvastatin or captopril (+3) more than omega 3 treated group (+2) and DOX treated group (+1). Bcl-X expression was not significantly affected in all treated group (Figure 6), no significant modification in the expression of Bcl-X was evident in tumors from DOX, CAP, ROV and OMEGA treated- groups as well as the DEN group.
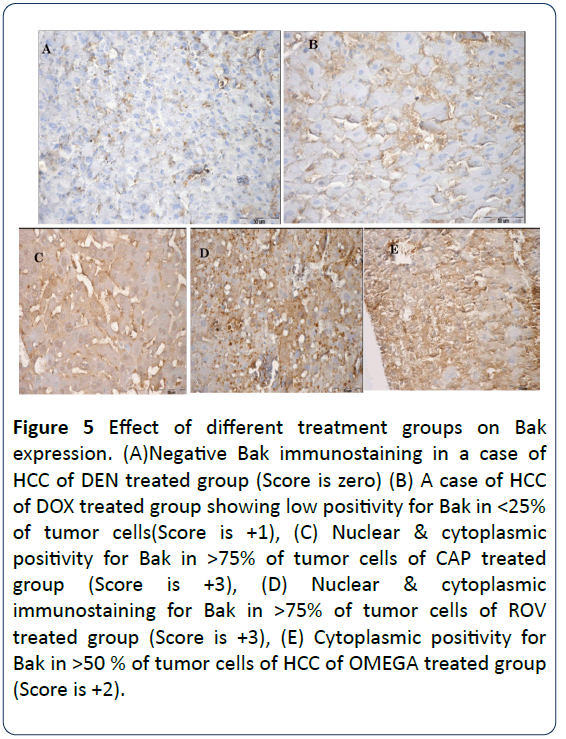
Figure 5: Effect of different treatment groups on Bak expression. (A)Negative Bak immunostaining in a case of HCC of DEN treated group (Score is zero) (B) A case of HCC of DOX treated group showing low positivity for Bak in <25% of tumor cells(Score is +1), (C) Nuclear & cytoplasmic positivity for Bak in >75% of tumor cells of CAP treated group (Score is +3), (D) Nuclear & cytoplasmic immunostaining for Bak in >75% of tumor cells of ROV treated group (Score is +3), (E) Cytoplasmic positivity for Bak in >50 % of tumor cells of HCC of OMEGA treated group (Score is +2).
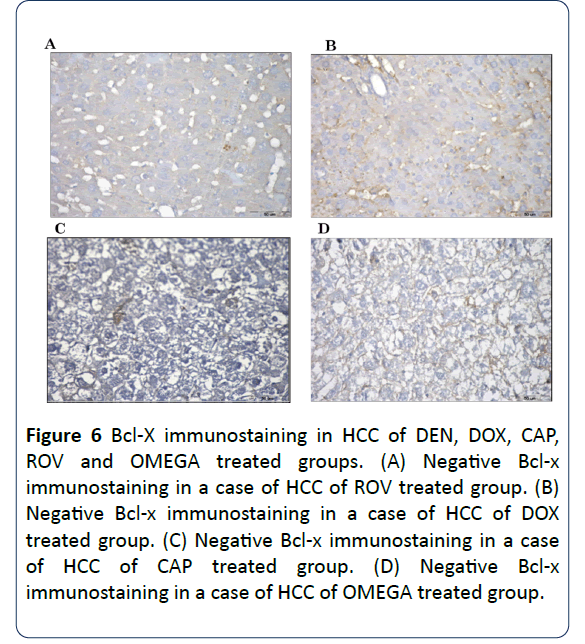
Figure 6: Bcl-X immunostaining in HCC of DEN, DOX, CAP, ROV and OMEGA treated groups. (A) Negative Bcl-x immunostaining in a case of HCC of ROV treated group. (B) Negative Bcl-x immunostaining in a case of HCC of DOX treated group. (C) Negative Bcl-x immunostaining in a case of HCC of CAP treated group. (D) Negative Bcl-x immunostaining in a case of HCC of OMEGA treated group.
Effect of different treatment regimens either doxorubicin alone or its combination with captopril, rosuvastatin or omega 3 on the percentage of heart weight /body weight ratio (HW/BW):
During the treatment period, the mortality rate was approximately 90% in the DOX group and approximately 50% in other groups CAP, ROV and 70% in OMEGA, all animals of DOX-treated group produced characteristic signs as dyspnea, enlarged abdomen, enlarged kidneys and liver, fluid accumulation in the peritoneal cavity, and animals looked weaker and lethargic. DOX-treated mice showed a significant loss in their heart weights and in the heart to body weight ratio (Figure 7). Addition of rosuvastatin, capoten or omega 3 to doxorubicin treatment significantly suppressed the reduction in heart weight as well as the decrease in the heart/ body weight ratio as compared to DOX-treated group.
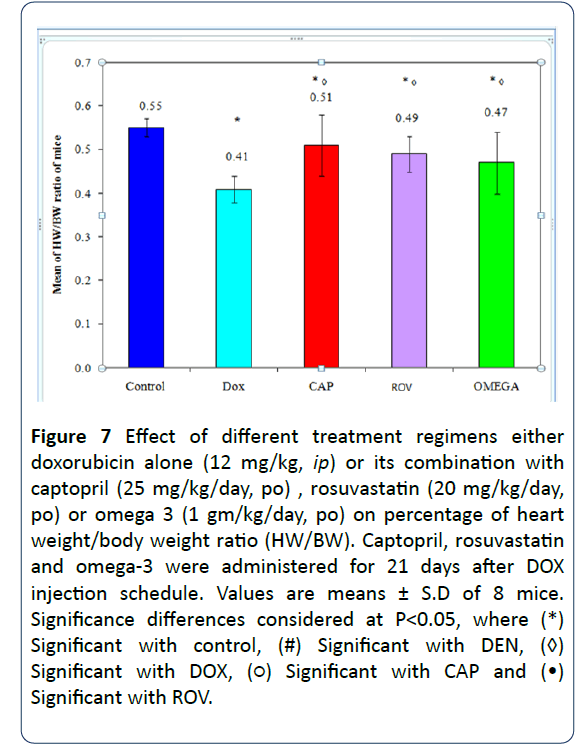
Figure 7: Effect of different treatment regimens either doxorubicin alone (12 mg/kg, ip) or its combination with captopril (25 mg/kg/day, po) , rosuvastatin (20 mg/kg/day, po) or omega 3 (1 gm/kg/day, po) on percentage of heart weight/body weight ratio (HW/BW). Captopril, rosuvastatin and omega-3 were administered for 21 days after DOX injection schedule. Values are means ± S.D of 8 mice. Significance differences considered at P?0.05, where (*) Significant with control, (#) Significant with DEN, (◊) Significant with DOX, (?) Significant with CAP and (•) Significant with ROV.
Effect of different treatment regimens either doxorubicin alone or its combination with captopril, rosuvastatin or omega 3 on H & E staining of mouse heart:
H & E staining of heart tissue sections of DOX treated group revealed cardiotoxicity of doxorubicin evidenced by degenerated necrotic purkinje fibers (absence nuclear staining). Addition of rosuvasatin or captopril or omega 3 to doxorubicin greatly lowered its cardiotoxicity (Figure 8).
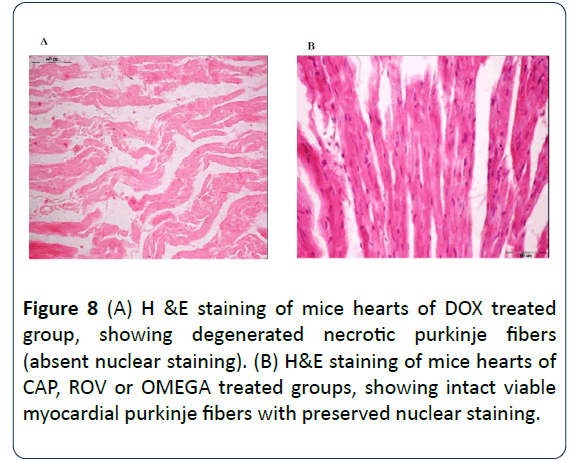
Figure 8: (A) H &E staining of mice hearts of DOX treated group, showing degenerated necrotic purkinje fibers (absent nuclear staining). (B) H&E staining of mice hearts of CAP, ROV or OMEGA treated groups, showing intact viable myocardial purkinje fibers with preserved nuclear staining.
Effect of different treatment regimens either doxorubicin alone or its combination with captopril, rosuvastatin or omega 3 on the level of TNF-α and oxidative stress markers in mouse heart:
The levels of TNF-α expressed in mice heart tissues of the different experimental groups are illustrated in Figure 9A. The level of TNFα was increased significantly in hearts of DOX - treated group in a comparison with the control group. In contrast, administration of captopril (25 mg/kg - oral), rosuvastatin (20 mg/kg- oral) or omega 3 (1 gm/kg - oral) resulted in a significant decrease in the level of cardiac TNF-α in mice compared to the DOX-treated group. The highest significant reduction was noticed in mice treated with captopril. However, there is no significant difference between ROV or OMEGA groups. Additionally, the level of reduced GSH level and SOD estimated in the heart of the different treated groups is illustrated in Figure 9B and 9C. A significant decrease in GSH and SOD levels were observed in DOX - treated group compared to the control group. All tested regimens including captopril, rosuvastatin or omega 3 showed a significant increase in cardiac GSH and SOD levels compared to the DOX - treated group. Noticeably, OMEGA group showed a marked increase in these levels that were significantly different from that of CAP or ROS groups. Furthermore, MDA level estimated in the heart of the different treated groups is shown in Figure 9D. The cardiac level of MDA was significantly increased in DOX - treated group when compared to the DEN group. However, addition of captopril or rosuvastatin significantly suppressed the increase in cardiac MDA level. Paradoxically, omega-3 treatment significantly increased MDA level as compared to DOX – treated group.
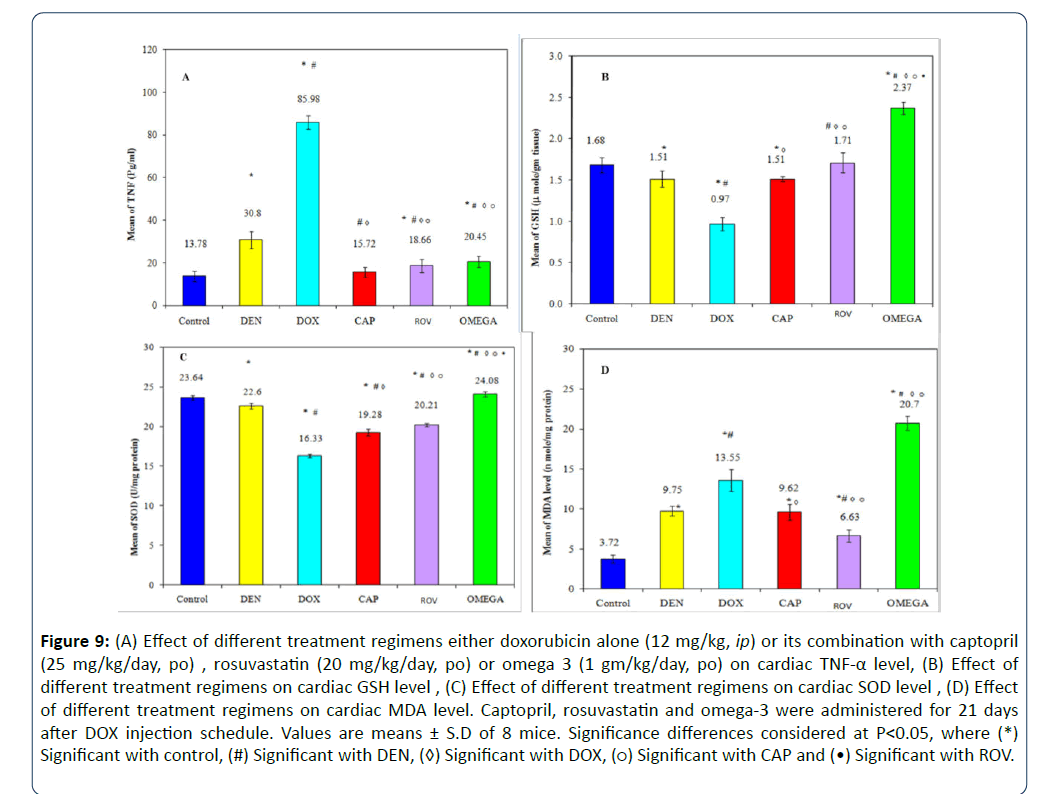
Figure 9: (A) Effect of different treatment regimens either doxorubicin alone (12 mg/kg, ip) or its combination with captopril (25 mg/kg/day, po) , rosuvastatin (20 mg/kg/day, po) or omega 3 (1 gm/kg/day, po) on cardiac TNF-α level, (B) Effect of different treatment regimens on cardiac GSH level , (C) Effect of different treatment regimens on cardiac SOD level , (D) Effect of different treatment regimens on cardiac MDA level. Captopril, rosuvastatin and omega-3 were administered for 21 days after DOX injection schedule. Values are means ± S.D of 8 mice. Significance differences considered at P?0.05, where (*) Significant with control, (#) Significant with DEN, (◊) Significant with DOX, (?) Significant with CAP and (•) Significant with ROV
Discussion
Despite its usefulness as anti-neoplastic agent, DOX like most of the anticancer drugs has several toxic effects; the most serious is the fatal cardiotoxicity and DOX-induced cardiomyopathy (DIC). One of the current goals in cancer therapy is to reduce the development the side effects of chemotherapy while maintaining its antitumoral capability. Our study has unique aspects because it is the first to report the ability of rosuvastatin to potentiate the antitumoral effect of DOX. To the best of our knowledge, it is also the first investigation comparing the antitumoral and cardioprotective effects, of (ROV, CAP and Omega 3) in combination with DOX.
Our findings support the hypothesis that combined treatment is beneficial in ameliorating DOX-induced cardiac damage with increment of its antitumoral efficacy within the therapeutic range. More favorable results were obtained in ROV and CAP groups. Interestingly, our results provided important information on how ROS and CAP decreased DIC more than Omega did.
The present data showed that all three drugs; ROV,CAP and OMEGA enhanced the antitumoral effect of DOX by decreasing tumor cell viability, increasing the number of apoptotic cells and the intensity of Bak expression (pro apoptotic protein) and decreased VEGF in comparison with DOX- treated mice. As regards ROV, our data are in agreement with Anna Martirosyan et al. [35] who found that lovastatin increased the apoptotic effect of doxorubicin in tumor cells through inhibiting of P glycoprotein (P-gp) in multi-drug resistance (MDR) tumor cells and blocking mevalonate pathway depending on HMG-COA reductase inhibition [36]. In the present study, it is noteworthy to mention that ROV was shown to have an antiangiogenic effect which is in agreement with Tijeras-Raballand et al. [37] who found that ROV counteracted vessel arterialisation and sinusoid capillarisation in murine HCC.
Our data showed that CAP decreased VEGF level and tumor cell viability significantly compared to doxorubicin treated group. Captopril was established as anti-cancer drug and decreased the progression of hepatocarcinogenesis [38]. The most accepted explanation for this finding is that previous studies have revealed local expression of several components of the renin angiotensin system (RAS) in various cancer cells and tissues [38-40]. Scientists have shown that angiotensin II can increase cell proliferation and migration, as well as angiogenesis, in several experimental models [40]. Imanishi et al. [41] even proved that the level of VEGF was increased due to the proangiogenic activity of angiotensin II on AT1R in endothelial cells. Captopril may also have other mechanisms for its antitumor activity such as reaction with matrix metalloproteases (MMPs). Prontera et al. [42] reported that captopril can reduce tumor growth and lung metastases in mice bearing Lewis lung carcinoma, by inhibiting MMP-2.
It is likely that suppression of tumor cell growth by (n-3) fatty acids is due to the combination of several mechanisms rather than a single one. The level of VEGF decreased significantly in OMEGA group compared to DOX-treated group, but was less significant than CAP and ROV- treated groups. This finding is in agreement with Nuria Matesanz et al. [43] who declared that docosahexanoic acid (DHA) reduced VEGFmediated angiogenic signaling in microvascular endothelial cells. However, the activity of VEGF is dependent on free radical production, namely the production of endothelial nitric oxide synthetase (eNOS) and NADPH oxidase–derived NO and O2−, which act as second messengers to stimulate migration, proliferation, and angiogenesis [44-46]. The role of ω-3 polyunsaturated fatty acids (PUFAs) in modifying these VEGFmediated signaling cascades might be through anti-oxidant effect of omega 3.
The aforementioned information fulfilled the primary objective of the present study which is enhancing the antitumor effect of DOX. Our second goal was to examine a new therapeutic combination with doxorubicin, reducing its cardiotoxicity. Noteworthy, the mortality rate during treatment was approximately 90% and 70% in the DOX-treated and OMEGA- treated groups, respectively, while mortality was approximately 50% in CAP and ROV groups. All animals of DOXtreated group produced characteristic signs as dyspnea, enlarged abdomen, enlarged kidneys and liver, fluid accumulation in the peritoneal cavity, and animals looked weaker and lethargic, these clinical signs and symptoms were markedly reduced in all treated groups. DOX-induced cardiotoxicity and oxidative stress relationship has been confirmed in our study by myocardial cell damage, alteration in oxidative stress markers and elevation in TNF-α as an inflammatory mediator involved in cardiotoxicity of DOX.
Administration of our probed drugs concurrently with DOX markedly attenuated DOX-induced oxidative cardiac injury in mice as confirmed by significant increase in heart weight/body weight ratio, the level of cardiac GSH, SOD activity and a significant reduction in the level of TNF- α as compared to DOX- treated group. Similarly, CAP and ROV treatment significantly reduced the level of MDA. In addition, they caused relative normalization in myocardial histopathological examination evidenced by intact viable myocardial purkinje fibers with preserved nuclear staining. Paradoxically, MDA level was elevated following omega 3 treatments.
Remarkably, the role of antioxidative properties as a major underlying cause of cardiotoprotection has been recognized. Pertinent to this view are the observations; rosuvastatin possesses antioxidant and cardioprotective effects against DOX (Kim YH et al) [47], in addition to holding an apoptotic effect in the heart against DOX- induced cardiotoxicity (Sharma, et al.) [48]. In addition, statins inhibit the expression of TNF-α in particular, which is enhanced in various pathophysiological states, associated with increased oxidative stress [49].
Our study provided evidence that CAP ameloriated the development of DOX- induced cardiotoxicity. This is in line with the results of Van Gilst et al. [50] who reported that the ventricular fibrillation and the loss of high energy phosphate nucleotides following ischemia and reperfusion in isolated rat hearts are decreased by captopril. The explanation for our observation might be that captopril possesses a sulphydryl group and can be converted into disulphides through the interaction with free radicals instead of cellular sulphydrylcontaining proteins and enzymes [51]. In the current study captopril was shown to have an anti-inflammatory effect by reducing the level of TNF –α. These results are in agreement with several reports [51-53].
Interestingly, the reduction in mortality rate in the OMEGAtreated group was less than CAP and ROV- treated groups. Some animals of OMEGA group looked weaker and lethargic and had fluid accumulation in the peritoneal cavity. Carbone et al. [54] found that dietary intake of omega-3 PUFA failed to prevent and may indeed exacerbate DOX-induced cardiotoxicity. In contrast, Hrelia et al. [55] found that highly unsaturated fatty acids biosynthesis played a role in counteracting DOX toxicity, but it cannot completely overcome this cardiotoxicity. Our result can be explained by the fact that PUFAs create oxidative damage in biological system such as peroxyl and alkoxyl radicals. Therefore, we can postulate that omega-3 polyunsaturated fatty acids (n-3 PUFAs) may limit oxidative stress by increasing antioxidant capacity. Noteworthy, omega 3 induced a selective increase of lipid peroxidation (LPO) in tumor cells [56]. This selectivity might result from a differential handling of oxidative stress between tumor and non-tumor tissues [56]. It was reported that omega 3 enhances specifically the cytotoxicity of anthracyclines toward tumor cells without affecting normal cells, like cardiomyocytes [56]. It is unclear if the cardioprotective effect is attributed to a suppression of the oxidative stress induced by doxorubicin , because omega 3 exhibited a less cardioprotective effect despite its antioxidant effect and this is in agreement with Kim et al. [47] who found that, carvidilol did not exhibit cardioprotective effect despite its antioxidant effect .
In our study, Omega 3 has been shown to have an antiinflammatory action, it decreased the level of TNF -α in hearts of mice when compared to DOX group, these data are in accordance with Pischon et al. [57]. The biochemical pathways supporting the putative anti-inflammatory effects of n-3 fatty acids may be through enrichment of membrane phospholipids; EPA competes with arachidonic acid as a substrate for the production of cycloxygenase- and lipoxygenase-derived eicosanoids [58].
In summary, this study is a comparative investigation of the therapeutic use of ROV, CAP, or Omega 3 for the first time in combination with low dose of DOX, to enhance antitumor and apoptotic effects in chemotherapy of HCC. These combination treatments could fulfill the ever present aim of cancer treatment; to achieve an optimal antitumoral effect with minimal toxicity, effectively “killing two birds with one stone”. Since the pharmacokinetics and pharmacodynamics of these drugs are well characterized, it is foreseeable that they could be incorporated in combination with cytotoxic drugs into phase I clinical trials in the near future.
Limitation of the Study
The mortality rate after DEN or DOX administration was very high so a large number of animals were used. Additionally, the expression of Bcl-x was not changed after administration of our drugs.
Competing Interests
None
Authors’ Contributions
Eman selimah: Research idea, experimental design, data analysis and presentation, manuscript preparation and work supervision.
Ibrahim El-Sayed: performing the experiments, data analysis and manuscript preparation.
References
- Benvegnù L, Gios M, Boccato S, Alberti A (2004) Natural history of compensated viral cirrhosis: a prospective study on the incidence and hierarchy of major complications. Gut 53: 744-749.
- Sangiovanni A, Prati GM, Fasani P (2006) The natural history of compensated cirrhosis due to hepatitis C virus: a 17-year cohort study of 214 patients. Hepatology 43: 1303-1310.
- Besheer T, El-Bendary M, Elalfy H, Abd El-Maksoud M, Salah M, et al. (2017) Prediction of fibrosis progression rate in patients with chronic hepatitis C genotype 4: role of cirrhosis risk score and host factors. J Interferon Cytokine Res 37: 97-102.
- Besheer T, Arafa M, El-Maksoud MA, Elalfy H, Hasson A, et al. (2018) Diagnosis of cirrhosis in patients with chronic hepatitis C genotype 4: Role of ABCB11 genotype polymorphism and plasma bile acid levels. Turk J Gastroenterol 29: 299-307.
- Ferrara N, Kerbel RS (2005) Angiogenesis as a therapeutic target. Nature 438: 967-974.
- Kim KJ, Li B, Winer J, Armanini M, Gillett N, et al. (1993) Inhibition of vascular endothelial growth factor induced angiogenesis suppresses tumour growth in vivo. Nature 362: 841-844.
- Beerheide W, Tan YJ, Teng E, Ting AE, Jedpiyawongse A, et al. (2000) Downregulation of proapoptotic proteins Bax and Bcl-X(S) in p53 overexpressing hepatocellular carcinomas. Biochem Biophys Res Commun 273: 54-61.
- Shan K, Lincoff AM, Young JB (1996) Anthracycline-induced cardiotoxicity Ann. Intern Med 125: 47-58.
- Frederick CA, Williams LD, Ughetto G (1990) Structural comparison of anticancer drug-DNA complexes: adriamycin and daunomycin. Biochemistry 29: 2538-2549.
- Swain SM, Whaley FS, Gerber MC, Weisberg S, York M, et al. Cardioprotection with dexrazoxane for doxorubicin-containing therapy in advanced breast cancer. J Clin Oncol 15: 1318-1332.
- Minotti G, Menna P, Salvatorelli E, Cairo G, Gianni L (2004) Anthracyclines: molecular advances and pharmacologic developments in antitumor activity and cardiotoxicity. Pharmacol Rev 56: 185-229.
- Qu HY, Xiao YM, Jiang GH, Wang ZY, Zhang Y, et al. (2009) Effect of atorvastatin versus rosuvastatin on level of serum lipids. Pharma Res 26: 958-964.
- Weis M, Heeschen C, Glassford AJ, Cooke JP (2002) Statins have biphasic effects on angiogenesis. Circulation 105: 739-745.
- Luvai A, Mbagaya W, Hall AS, Barth JH (2012) Rosuvastatin: a review of the pharmacology and clinical effectiveness in cardiovascular disease. Clin Med Insights Cardiol 6:17-33.
- El- Mesery ME, Al-Gayyar MM, Salem HA, Darweish MM, El-Mowafy AM (2009) Chemo preventive and renal protective effects for docosahexaenoic acid (DHA): implications of CRP and lipid peroxides. Cell Div 4:6.
- Spencer L, Mann C, Metcalfe M, Webb MB, Pollard C, et al. (2009) The effect of omega-3 FAs on tumor angiogenesis and their therapeutic potential. Eur J Cancer 45: 2077-2086.
- Hori K, Saito S, Takahashi H, Sato H, Maeda H, et al. (2000) Tumor-selective blood flow decrease induced by an angiotensin converting enzyme inhibitor, temocapril hydrochloride. Jpn J Can Res 91: 261-269.
- Kardum D, Huskic J, Fabijanic D, Banic M, Buljevac M, et al. (1999) Activity of serum angiotensin-converting enzyme as a tumor marker of hepatocellular carcinoma. Eur J Gastroenterol Hepatol 11: 209-213.
- Shiota G, Harada K, Ishida M, Tomie Y, Okubo M, et al. (1999) Inhibition of hepatocellular carcinoma by glycyrrhizin in diethylnitrosamine-treated mice. Carcinogenesis 20: 59-63.
- Alshabanah OA, Hafez MM, Al-Harbi MM, Hassan ZK, Al Rejaie SS, et al. (2010) Doxorubicin toxicity can be ameliorated during antioxidant L-carnitine supplementation. Oxid Med Cell Longev 3: 428-433.
- Qiu Z, Zhang W, Fan F, Li H, Wu C, et al. (2012) Rosuvastatin-attenuated heart failure in aged spontaneously hypertensive rats via PKCalpha/beta2 signal pathway. J Cell Mol Med 16: 3052-3061.
- Calviello G, Palozza P, Di Nicuolo F, Maggiano N, Bartoli (2000) GMn-3 PUFA dietary supplementation inhibits proliferation and store-operated calcium influx in thymoma cells growing in Balb/c mice. J Lipid Res 41:182-189.
- Wysocki PJ, Kwiatkowska EP, Kazimierczak U, Suchorska W, Kowalczyk DW, et al. (2006) Captopril, an angiotensin-converting enzyme inhibitor, promotes growth of immunogenic tumors in mice. Clin Cancer Res 12: 4095-4102.
- Jakate S, Giusto D (2012) Pathology of Hepatocellular Carcinoma: Primary Liver Cancer. Humana Press, Totowa, NJ, USA..
- Edmondson HA, Steiner PE (1954) Primary carcinoma of the liver. A study of 100 cases among 48,900 necropsies. Cancer 7:462-503.
- Mathonnet M, Descottes B, Valleix D, Labrousse F, Truffinet V, et al. (2006) Quantitative analysis using ELISA of vascular endothelial growth factor and basic fibroblast growth factor in human colorectal cancer, liver metastasis of colorectal cancer and hepatocellular carcinoma. World J Gastroenterol 123: 3782-3783.
- Hsu SM, Raine L, Fanger H (1981) Use of avidin-biotin-peroxidase complex (ABC) in immunoperoxidase techniques: a comparison between ABC and unlabeled antibody (PAP) procedures. J Histochem Cytochem 29: 577-580.
- Li S, Yao D, Wang L, Wu W, Qiu L, et al. (2011) Expression characteristics of hypoxia-inducible factor-1α and its clinical values in diagnosis and prognosis of hepatocellular carcinoma. Hepatitis Monthly 11: 821-828.
- Kleeberger CA, Lyles RH, Margolick JB? Rinaldo CR, Phair JP, et al. (1999) Viability andrecovery of peripheral blood mononuclear cells cryopreserved for up to 12 years in a multicenter study. Clin Diagn Lab Immunol 6: 14-19.
- van der Poll T, Coyle SM, Barbosa K, Braxton CC, Lowry SF (1996) Epinephrine inhibits tumor necrosis factor-alpha and potentiates interleukin 10 production during human endotoxemia. J Clin Invest 97:713-719.
- Mihara M, Uchiyama M (1978) Determination of malonaldehyde precursor in tissues by thiobarbituric acid test. Anal Biochem 86: 271-278.
- Yamazaki S (1967) [Thiobarbituric acid (TBA) method]. Rinsho Byori 15:616-619.
- Richardson RJ, Murphy SD (1975) Effect of glutathione depletion on tissue deposition of methylmercury in rats. Toxicol Appl Pharmacol 31: 505-519.
- Marklund S, Marklund G (1974) Involvement of the superoxide anion radical in the autoxidation of pyrogallol and a convenient assay for superoxide dismutase. Eur J Biochem 47: 469-474.
- Martirosyan A, Clendening JW, Goard CA, Penn LZ (2010) Lovastatin induces apoptosis of ovarian cancer cells and synergizes with doxorubicin: potential therapeutic relevance. BMC Cancer 10:103.
- Liao JK, Laufs U (2005) Pleiotropic effects of statins. Annu Rev Pharmacol Toxicol 45: 89-118.
- Tijeras-Raballand A, Hainaud-Hakim P, Contreres JO, Gest C, Le Henaff C, et al. (2010) Rosuvastatin counteracts vessel arterialisation and sinusoid capillarisation, reduces tumour growth, and prolongs survival in murine hepatocellular carcinoma. Gastroenterol Res Pract 2010: 640797.
- Miyajima A, Kosaka T, Asano T, Seta K, Kawai T, et al. (2002) Angiotensin II type I antagonist prevents pulmonary metastasis of murine renal cancer by inhibiting tumor angiogenesis. Cancer Res 62: 4176-4179.
- Paul M, Poyan Mehr A, Kreutz R (2006) Physiology of local renin-angiotensin systems. Physiol Rev 86: 747-803.
- Suganuma T, Ino K, Shibata K, Kajiyama H, Nagasaka T, et al. (2005) Functional expression of the angiotensin II type 1 receptor in human ovarian carcinoma cells and its blockade therapy resulting in suppression of tumor invasion, angiogenesis, and peritoneal dissemination. Clin Cancer Res 11: 2686-2694.
- Imanishi T, Hano T, Nishio I (2004) Angiotensin II potentiates vascular endothelial growth factor-induced proliferation and network formation of endothelial progenitor cells. Hypertens Res 7: 101-108.
- Prontera C, Mariani B, Rossi C, Poggi A, Rotilio D (1999) Inhibition of gelatinase A (MMP-2) by batimastat and captopril reduces tumor growth and lung metastases in mice bearing Lewis lung carcinoma. Int J Cancer 81: 761-766.
- Matesanz N, Park G, McAllister H, Leahey W, Devine A, et al. (2010) Docosahexaenoic acid improves the nitroso-redox balance and reduces VEGF-mediated angiogenic signaling in microvascular endothelial cells. Invest Ophthalmol Vis Sci 51: 6815-6825.
- El-Remessy AB, Al-Shabrawey M, Platt DH (2007) Peroxynitrite mediates VEGF's angiogenic signal and function via a nitration-independent mechanism in endothelial cells. Am J Pathol 21: 2528-2530.
- Hardman WE, Moyer MP, Cameron IL (2000) Dietary fish oil sensitizes A549 lung xenografts to doxorubicin chemotherapy. Cancer Lett 151: 145-151.
- Sawada N, Inoue M, Iwasaki M, Sasazuki S, Shimazu T, et al. (2012) Consumption of n-3 fatty acids and fish reduces risk of hepatocellular carcinoma. Gastroenterol 142: 1468-1475
- Kim YH, Park SM, Kim M, Kim SH, Lim SY, et al. (2010) Cardioprotective effects of rosuvastatin and carvedilol on delayed cardiotoxicity of doxorubicin in rats. Toxicol Mech Methods 22: 488-498.
- Sharma H, Pathan RA, Kumar V, Javed S, Bhandari U (2011) Antiapoptotic potential of rosuvastatin pretreatment in murine model of cardiomyopathy. Int J Cardiol 150: 193-200.
- Mital S, Zhang X, Zhao G, Bernstein RD, Smith CJ, et al. (2000) Simvastatin up-regulates coronary vascular endothelial nitric oxide production in conscious dogs. Am J Physiol 279: H2649- H2657.
- Van-Gilst WH, De-Graeff PA, Kingma JH, Wesseling H, De-Langen CD (1984) Captopril reduces purine loss and reperfusion arrhythmias in the rat heart after coronary artery occlusion. Eur J Pharmacol 100: 113-117.
- Fouad AA, Jresat I (2013) Captopril and telmisartan treatments attenuate cadmium-induced testicular toxicity in rats. Fundam Clin Pharmacol 27: 152-160.
- Odaka C, Mizuochi T (2000) Angiotensin-converting enzyme inhibitor captopril prevents activation-induced apoptosis by interfering with T cell activation signals. Clin Exp Immunol 121:515-522.
- Schindler R, Dinarello CA, Koch KM (1995) Angiotensin-converting-enzyme inhibitors suppress synthesis of tumour necrosis factor and interleukin 1 by human peripheral blood mononuclear cells. Cytokine 7: 526-533.
- Carbone A, Psaltis PJ, Nelson AJ, Metcalf R, Richardson JD, et al. (2012) Dietary omega-3 supplementation exacerbates left ventricular dysfunction in an ovine model of anthracycline-induced cardiotoxicity. J Card Fail 18: 502-511.
- Hrelia S, Bordoni A, Biagi PL (2001) Role of gamma-linolenic acid in counteracting doxorubicin-induced damage in cultured rat cardiomyocytes. Prostaglandins Leukot Essent Fatty Acids 64: 139-145.
- Hajjaji N, Besson P, Bougnoux P (2012) Tumor and non-tumor tissues differential oxidative stress response to supplemental DHA and chemotherapy in rats. Cancer Chemother Pharmacol 70: 17-23.
- Pischon T, Hankinson SE, Hotamisligil GS, Rifai N, Willett WC, et al. (2003) Habitual dietary intake of n-3 and n-6 fatty acids in relation to inflammatory markers among US men and women. Circulation 108: 155-160.
- Simopoulos AP (2002) The importance of the ratio of omega-6/omega-3 essential fatty acids. Biomed Pharmacother 56: 365-379.

