Mohammad Hussein1, Eugene Mech2*, Ahmed Bakry2, Lisa VanHouwelingen3, Mark Walton J3, Elyanne Ratcliffe1 and Robert Issenman1
1Department of Pediatric Gastroenterology and Hepatology, McMaster Children’s Hospital, Hamilton Health Sciences, Hamilton, ON, Canada
2Department of Gastroenterology, McMaster University, Hamilton, ON, Canada
3Department of Pediatric Surgery, McMaster Children’s Hospital, Hamilton Health Sciences, Hamilton, ON, Canada
*Corresponding Author:
Eugene Mech
Department of Gastroenterology, McMaster
University, 1200 Main St. West, Hamilton
Ontario, Canada
Tel: + 289-795-3469
E-mail: meche@mcmaster.ca
Received Date: November 04, 2017 Accepted Date: November 07, 2017 Published Date: November 09, 2017
Citation: Hussein M, Mech E, Bakry A, VanHouwelingen L, Walton JM, et al. (2017) Pediatric Duodenal Dieulafoy’s Lesion, A Serious but Rare Condition: Case Report and Literature Review. J Clin Gastroenterol Hepatol Vol.1: No. 4: 27. doi: 10.21767/2575-7733.1000027
Keywords
Children; Dieulafoy’s lesion; Upper gastrointestinal bleed; Gastric; Duodenal
Introduction
Dieulafoy’s lesion refers to gastrointestinal ulcer as first described in 1897 with erosion of a superficial large-caliber artery and massive bleeding [1]. This lesion has been recognized as an important cause of obscure upper gastrointestinal hemorrhage [2]. It accounts for approximately 2% of acute upper gastrointestinal bleeding. The lesion is characterized by a minute mucosal defect, with a large and tortuous artery at the base, causing the artery to rupture with potentially life-threatening bleeding. The mainstay of treatment of this lesion remains radiologic arterioembolization. We report a case where surgical intervention was required to stop the bleeding after endoscopic and angiographic interventions failed.
Methodology
A review of the literature was conducted using the OVID Medline online database. The search was conducted with the following search terms: children, Dieulafoy’s lesion, upper gastrointestinal bleed, gastric, duodenal. Relevant articles, abstracts, and their references were reviewed.
Case Report
A 16-year-old male, with a history of high-risk Acute Lymphoblastic Leukemia (ALL), who had recently completed a course of high dose methotrexate as part of his consolidation 1 phase, developed a massive Gastrointestinal (GI) bleed. Over the previous two days, the patient had two syncopal/ presyncopal episodes which were attributed to the chemotherapy induced anemia. The patient developed melena overnight, complained of abdominal pain and one episode of non-bloody emesis. A pantoprazole infusion was initiated, and he was transferred to the ICU. In the ICU, the patient received 8 units of blood over the ensuing 24 hours. Steroid therapy was discontinued as a potential contributor to possible gastritis.
On physical examination, the patient was observed to be obese (BMI of 30.9), afebrile, tachycardic (HR of 146), and hypotensive with a systolic blood pressure of 66. There was no rash or petechiae. The abdomen was soft, tender but not distended. Normal bowel sounds were observed without evident hepatosplenomegaly. Laboratory studies indicated a hemoglobin of 53, a white blood cell count of 3.2 and ANC of 1200, creatinine of 40, BUN of 10, Bilirubin of 35, and high transaminases; ALT was 406 and AST was 145. Stool cultures were positive for C. difficile.
The first esophagogastroduodenoscopy (EGD) to 22 cm showed both fresh and old blood with an intact looking mucosa after three water flushes. However, the bleeding lesion was not identified. Therefore, a flexible recto sigmoidoscopy with a second EGD was organized.
During the second endoscopy, a non-bleeding ulcer was noted at the gastroesophageal junction and a clot was noted at the gastric fundus. The stomach was observed to be filled with blood. A gush of bright red blood was encountered upon entering the second and third part of the duodenum, (Figure 1). An actively bleeding arterial vessel was noted. Angioembolization of the gastro-duodenal artery and the superior and inferior pancreaticoduodenal arteries failed to arrest the bleeding. The patient had received over 60 units of packed red blood cells, 12 units of FFP, and 8 units of platelets; the decision was made to proceed to laparotomy.
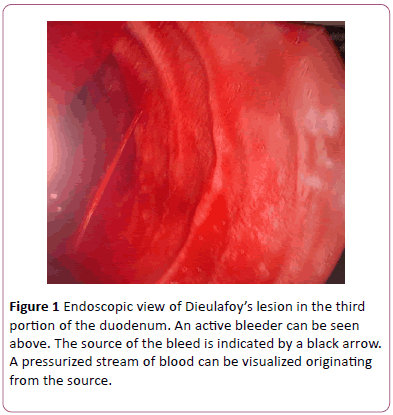
Figure 1: Endoscopic view of Dieulafoy’s lesion in the third portion of the duodenum. An active bleeder can be seen above. The source of the bleed is indicated by a black arrow. A pressurized stream of blood can be visualized originating from the source.
Intraoperative esophagogastroduodenoscopy (EGD) procedure confirmed the lesion to be at the third portion of the duodenum. A duodenotomy was performed. Once the duodenum was opened, the actively bleeding vessel could not be identified despite tattoo of the bleeding site during the second endoscopy. An unusual mucosal fold was felt to be the probable site of the Dieulafoy’s lesion and was over sewn. No further bleeding was noted, and the patient survived.
Discussion
Dieulafoy’s lesion usually occurs within 6 cm. of the gastroesophageal junction. These are principally found on the lesser curvature possibly a result of the unique vasculature of the stomach in this region [2]. Nine hundred cases of upper GI bleeding have been investigated in one large study in India; Dieulafoy’s lesion was found to be the cause in only six (0.67%) cases. The lesion was located within 6 cm of the GE junction in all cases [3]. Extragastric Dieulafoy’s lesion have rarely been reported. Veldhuyzen et al. could not find any duodenal lesions upon reviewing 100 cases of Dieulafoy’s lesion [4].
Duodenal Dieulafoy’s lesion was reported for the first time in 1988 [5]. Dieulafoy’s like lesion have also been described in the esophagus [6,7], jejunum, colon, and rectum [7-9]. Extragastric Dieulafoy’s lesion are being identified more frequently with increasing awareness of the condition [7,8]. In a large series of 89 patients with Dieulafoy’s lesion almost one third of the cases had extragastric Dieulafoy’s lesion. The duodenum was the commonest site with (14%-18%) extragastric locations, followed by the colon (5%-10%), jejunum (1%-2%), and esophagus (1%-2%) [7].
Since the evolution of the term ‘Dieulafoy’s lesion’, endoscopy has been the mainstay in its diagnosis and treatment. Specific endoscopic criteria have been developed in order to help diagnose and define Dieulafoy’s lesion:
• Active arterial spurting or micro pulsatile streaming from a minute mucosal defect or through normal surrounding mucosa.
• Visualization of a protruding vessel with or without active bleeding within a minute mucosal defect or through normal surrounding mucosa.
• Fresh, densely adherent clot with a narrow point of attachment to a minute mucosal defect or to normal appearing mucosa [9].
In the case reported, it would have been difficult to diagnose the lesion unless the patient was actively bleeding during the procedure (Figure 1). The second endoscopy further into the duodenum, to D2/D3, visualized the bleeding vessel (Figure 1). Dieulafoy’s lesion is an extremely difficult lesion to diagnose and should be considered during evaluation of any patient with recurrent massive GI bleeding [2,5]. More extensive investigation should be taken in the absence of a history of NSAID ingestion, peptic ulcer disease, alcohol abuse, or steroid intake [2,5]. In our case, steroids were discontinued as a potential contributor to the bleeding.
Endoscopy has aided the early diagnosis of the Dieulafoy’s lesion. Old reports have shown that only 50% of the Dieulafoy’s lesions were diagnosed at the initial endoscopy, whereas one third of the lesions required repeated endoscopy. The remainder were identified in the operating room or on angiography. More recent reports indicate that over 90% of cases have been identified at the first endoscopic intervention due to both the increase in awareness of the pathology as well as the careful endoscopic evaluation [2].
Therapeutic endoscopy has been the mainstay in the management of Dieulafoy’s lesion [2,7,10,11]. Adrenaline injection has been first used as sole therapy or combined with other endoscopic modalities which failed to control the bleeding in our case. The other endoscopic hemostatic techniques include:
• Bipolar and monopolar electrocoagulation
• Heater probe
• Laser photocoagulation
• Injection sclerotherapy
• Hemoclipping and Endoscopic Band Ligation (EBL) [1,6,9]. Hemoclipping was attempted in our case but the clips did not deploy due to the awkward position of the lesion.
Electrocoagulation and thermocoagulation methods should be avoided with duodenal Dieulafoy’s lesion due to the risk of transmural injury of the relatively thin walled duodenum [2].
The following techniques have shown to be safer and more effective:
• Vascular clips, as the normal surrounding mucosa in a Dieulafoy’s lesion makes it an adequate target for hemoclipping [12,13].
• Endoscopic Band Ligation (EBL), as a simple and inexpensive method for the treatment of Dieulafoy’s lesion [11,14].
Mechanical techniques have shown superiority over the injection methods in a comparative study in terms of both bleeding control as well as recurrence prevention [15]. Finally, surgery with ligation can provide the last resort for bleeding control upon failure of endoscopic intervention [2,5,11]. For poor surgical candidates with active bleeding, angiography and embolization could be considered as the modality of choice [16].
Conclusion
Pediatric duodenal Dieulafoy’s lesion is a recognized cause of upper gastrointestinal bleeding. Although rare, it is important to consider this GI bleed in the differential diagnosis of recalcitrant upper gastrointestinal bleeding. Early considerations of this anomaly will likely lead to earlier diagnosis; which will avoid unnecessary intervention, utilize cost-effective treatments, and decrease morbidity and mortality.
References
- Senger JL, Kanthan R (2012) The evolution of Dieulafoy's lesion since 1897: Then and now-A journey through the lens of a pediatric lesion with literature review. Gastroenterol Res Pract 2012: 432517.
- Al-Mishlab T, Amin AM, Ellul JM (1999) Dieulafoy's lesion: An obscure cause of GI bleeding. J R Coll Surg Edinb 44: 222-225.
- Arora A, Mehrotra R, Patnaik PK, Pande G, Ahlawat S, et al. (1991) Dieulafoy's lesion: A rare cause of massive upper gastrointestinal haemorrhage. Trop Gastroenterol 12: 25-30.
- Veldhuyzen Van Zanten SJ, Bartelsman JF, Schipper ME, Tytgat GN (1986) Recurrent massive hematemesis from Dieulafoy vascular malformation- A review of 101 cases. Gut 27: 213-222.
- McClave SA, Goldschmid S, Cunningham JT, Boyd WP Jr (1988) Dieulafoy's cirsoid aneurysm of the duodenum. Dig Dis Sci 33: 801-805.
- Ertekin C, Barbaros U, Taviloglu K, Guloglu R, Kasoglu A (2002) Dieulafoy's lesion of esophagus. Surg Endosc 16: 219.
- Norton ID, Petersen BT, Sorbi D, Balm RK, Alexander GL, et al. (1999) Management and long-term prognosis of Dieulafoy lesion. Gastrointest Endosc 50: 762-767.
- Gadenstatter M, Wetscher G, Crookes PF, Mason RJ, Schwab G, et al. (1998) Dieulafoy's disease of the large and small bowel. J Clin Gastroenterol 27: 169-172.
- Dy NM, Gostout CJ, Balm RK (1995) Bleeding from the endoscopically-identified Dieulafoy lesion of the proximal small intestine and colon. Am J Gastroenterol 90: 108-111.
- Goldenberg SP, DeLuca VA Jr, Marignani P (1990) Endoscopic treatment of Dieulafoy's lesion of the duodenum. Am J Gastroenterol 4: 452-454.
- Nikolaidis N, Zezos P, Giouleme O, Budas K, Marakis G, et al. (2001) Endoscopic band ligation of Dieulafoy-like lesions in the upper gastrointestinal tract. Endoscopy 33: 754-760.
- Hokama A, Ikema R, Hanashiro K, Kinjo F, Saito A (1996) Endoscopic hemoclipping for duodenal Dieulafoy's lesion. Am J Gastroenterol 91: 2450.
- Sueoka N, Koizumi N, Inokuchi K, Wakabayashi I (1997) Combined endoscopic clipping and ethanol injection for treatment of Dieulafoy's lesions in the duodenum. Gastrointest Endosc 46: 574-575.
- Ertekin C, Taviloglu K, Barbaros U, Guloglu R, Dolay K (2002) Endoscopic band ligation: Alternative treatment method in nonvariceal upper gastrointestinal hemorrhage. J Laparoendosc Adv Surg Tech A 12: 41-45.
- Chung IK, Kim EJ, Lee MS, Kim HS, Park SH, et al. (2000) Bleeding Dieulafoy's lesions and the choice of endoscopic method: comparing the hemostatic efficacy of mechanical and injection methods. Gastrointest Endosc 52: 721-724.
- Katz PO, Salas L (1993) Less frequent causes of upper gastrointestinal bleeding. Gastroenterol Clin North Am 22: 875-889.

