Teppei Tokumaru1, Yasuo Shima1, Takehiro Okabayashi1*, Yuichi Saisaka1, Tatsuaki Sumiyoshi1, Kenta Sui1, Sojiro Morita2, Yasuhiro Shimada3 and Jun Iwata4
1Department of Gastroenterological Surgery, Kochi Health Sciences Center, Japan
2Department of Radiology, Kochi Health Sciences Center, Japan
3Department of Clinical Oncology, Kochi Health Sciences Center, Japan
4Department of Diagnostic Pathology, at Kochi Health Sciences Center, Japan
*Corresponding Author:
Takehiro Okabayashi
Department of Gastroenterological Surgery, Kochi Health Sciences Center, Ike 2125-1, Kochi-City, Kochi 781-8555, Japan
Tel: +81- 88-837-3000
Fax: +81- 88-837-6766
E-mail: tokabaya@gmail.com
Received date: April 04, 2017; Accepted date: April 17, 2017; Published date: April 19, 2017
Citation: Tokumaru T, Shima Y, Okabayashi T, et al. Multimodal Therapy for Pancreatic Neuroendocrine Tumors with Multiple Liver Metastases - Two Case Reports. J Clin Gastroenterol Hepatol 2017, 1: 2. doi: 10.21767/2575-7733.1000012
Keywords
Pancreatic neuroendocrine tumors; Liver metastasis; Surgery; Multimodal therapy; Outcomes
Introduction
Pancreatic neuroendocrine tumors (PNET) are rare tumors that consist of a diverse set of the pancreas [1,2]. PNET remain an important clinical issue due to the high incidence of metastatic rate, and the lack of an evidenced-based treatment strategy [3-6]. Liver is the most common place for PNET distance metastasis, and literature reports showed a 46% to 93% hepatic metastasis rate [7]. Considerable controversy exists regarding how best to manage patients with PNET with liver metastases, with some advocating an aggressive surgical approach, although several researchers reported that surgical treatment of liver metastases of PNET remains the only therapy with the potential for a cure [8]. We herein document two cases of patients suffering from PNETs with synchronous multiple liver metastases who successfully underwent aggressive surgical management.
Case Presentations
Case 1
A 45-year-old man with multiple liver mass detected by abdominal ultrasonography was referred for evaluation and treatment. The patient without any clinical symptoms was previously healthy with no history of heavy alcohol consumption, smoking, diabetes mellitus, and malignancy. Examination revealed no palpable mass in the abdomen, ascites, or superficial lymphadenopathy. Laboratory test results included following; carcinoembryonic antigen (CEA), 0.8 ng/mL (normal range, 0.0-5.0 ng/mL); carbohydrate antigen 19-9 (CA19-9), 10.2 (normal range, 0.0-37.0); neuronspecific enolase (NSE), 12.6 (normal range, 0.0-16.3).
Axial contrast-enhanced computed tomography (CECT) of a pancreatic tumor with calcification in the arterial phase shows a 2cm in diameter hypervascular mass in the pancreatic tail following with the enhancement pattern being retained in the delayed phase (Figure 1a). Gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid magnetic resonance imaging demonstrated that 29 dominant low-signal intense lesions in the whole l i v e r (Figure 1b). Under the diagnosis of PNET with synchronous multiple liver metastases, pancreaticosplenectomy for the primary PNET and aggressive hepatic resection for multiple liver metastases which were detected by intraoperative ultrasound sonography were performed. Histological findings obtained from the tumor showed round, uniform cells, with round uniform nuclei, arranged in nests, trabeculae, and gland-like formations. Immunohistochemistry showed positive findings for CD56, chromogranin A, and synaptophysin. Ki-67 labeling index was positive in 11.2% of tumor cells, and the mitotic count index (/10 HPF) was 2 (Figure 1c). The grade was PNET-G2 according to the WHO classification [9].
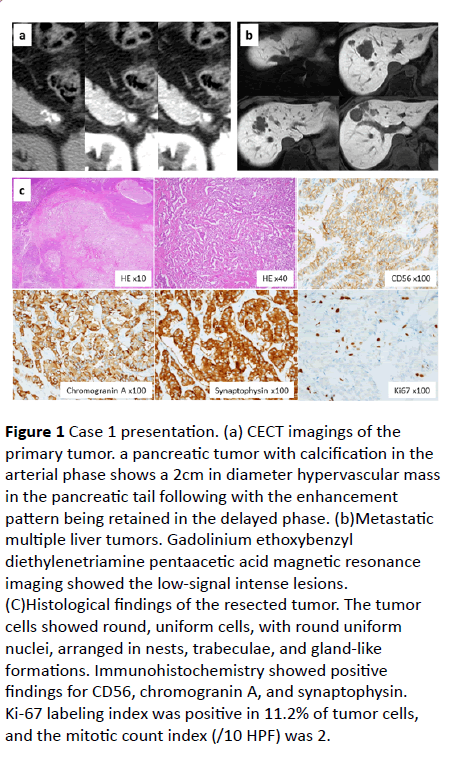
Figure 1 Case 1 presentation. (a) CECT imagings of the primary tumor. a pancreatic tumor with calcification in the arterial phase shows a 2cm in diameter hypervascular mass in the pancreatic tail following with the enhancement pattern being retained in the delayed phase. (b)Metastatic multiple liver tumors. Gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid magnetic resonance imaging showed the low-signal intense lesions. (C)Histological findings of the resected tumor. The tumor cells showed round, uniform cells, with round uniform nuclei, arranged in nests, trabeculae, and gland-like formations. Immunohistochemistry showed positive findings for CD56, chromogranin A, and synaptophysin. Ki-67 labeling index was positive in 11.2% of tumor cells, and the mitotic count index (/10 HPF) was 2.
The post-operative course was uneventful and transcatheter arterial chemoembolization (TACE) with epirubicin was performed for residual tumors of the remnant liver on postoperative day 16. He received long-acting somatostatin analogue from post-operative day 27 (30 mg/body weight every month) as an adjuvant setting. He is presently well without any evidence of recurrence 26 months after the operation.
Case 2
A 70-year-old man who was suffering from diarrhea for duration of one moth was diagnosed as pancreatic tail tumor with multiple liver mass and was referred to our hospital. There were no previous symptoms and he had no family history of malignant diseases. Physical examination showed normal body temperature, blood pressure, pulse rate, and respiratory rate. There was no superficial lymphadenopathy. Laboratory test results included following; CEA, 2.5 ng/mL; CA19-9, 10.0; NSE, 10.0; gastrin test, 1200 pg/mL (normal range, 40-140 pg/mL). Other laboratory tests, including hematology, nutritional status, and muscle enzymes, were within normal range.
There is a large mass in the tail of the pancreas that is hypervascular, unlike an adenocarcinoma, with peripheral enhancement and central necrosis in both arterial and delayed phase (Figure 2a). CECT revealed multiple focal hepatic lesions, consistent with metastases, that the masses are hypodense to background liver parenchyma. The masses demonstrate hyperdensity on arterial and portal phase, which visually does not allow the distinction between subtle washout and prolonged enhancement in a liver (Figure 2a). Microscopically, tumors are composed of round uniform cells with round uniform nuclei and immunohistochemical stains revealed positive findings for CD56, chromogranin A, and synaptophysin. Unfortunately, however, immunohistochemistry staining showed negative findings for gastrin. Ki-67 labeling index was positive in 11.4% of tumor cells, and the mitotic count index (/10 HPF) was 2 (Figure 2b).
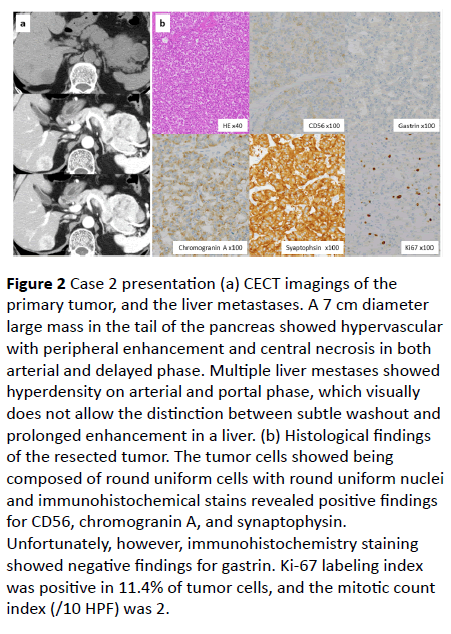
Figure 2 Case 2 presentation (a) CECT imagings of the primary tumor, and the liver metastases. A 7 cm diameter large mass in the tail of the pancreas showed hypervascular with peripheral enhancement and central necrosis in both arterial and delayed phase. Multiple liver mestases showed hyperdensity on arterial and portal phase, which visually does not allow the distinction between subtle washout and prolonged enhancement in a liver. (b) Histological findings of the resected tumor. The tumor cells showed being composed of round uniform cells with round uniform nuclei and immunohistochemical stains revealed positive findings for CD56, chromogranin A, and synaptophysin. Unfortunately, however, immunohistochemistry staining showed negative findings for gastrin. Ki-67 labeling index was positive in 11.4% of tumor cells, and the mitotic count index (/10 HPF) was 2.
Post-operative course was uneventful and diarrhea was improved after the operation. He received everolimus as an adjuvant setting orally once daily at a dose of 10 mg on day 1 through 28 of a 42-day cycle from post-operative day 30. The patient has been alive without any recurrence for 40 months since curative surgical treatment.
Discussion
PNET, formerly known as islet cell tumors, account for about 3% of primary pancreatic cancer [2,10]. Liver metastases accounts for about 90% of the distant metastases of PNET and is a major prognostic factor for this tumor [2,10,11]. Previous researchers have reoprted that the concurrent resection of both the primary lesion and resectable liver metastases is feasible and might improve the prognosis [3-6]. Palliative cytoreductive surgery refers to the removal of most of the metastasis (>90% of the lesion), during which the concurrent or staged resection of the primary lesion or liver metastases may be considered according to ENETS consensus guidelines [12].
In the recent years, PROMID study and RADIANT-3 Clinical Trial have reported that long-acting somatostatin analogue and everolimus can be effective of advanced PNETs as antitumor agents [13,14]. With the advancement of anti- tumor agents, multimodal therapy can improve the prognosis for PNETs. In the current series, one patient received long-acting somatostatin analogue 30 mg intramuscularly in monthly intervals according to the regimen of PROMID Study [13]. In another case, although everolimus was administered at orally daily at a dose of 10 mg once a day in the RADIANT-3, our case administered at a dose of 10 mg on day 1 through 28 of a 42- day cycle for preventing the adverse events [14].
Up to now no high-quality evidences has supported the application of adjuvant therapies might benefit PNET patients following curative resection. However, clinical research on the adjuvant therapies should be considered in patients at high risk of tumor relapse. Our results suggested that aggressive surgical resection with multimodal therapy for advanced PNETs with liver metastases might be effective in achieving long-term survival and both long-acting somatostatin analogue and everolimus might be useful as an adjuvant setting.
Conclusion
In conclusion, we successfully performed radical surgery for advanced PNET with multiple liver metastases. Furthermore, long-term survivals without any tumor recurrences were obtained by administrating adjuvant therapies. New avenues of individualized treatment may also be reached by the inclusion of molecular parameters of the tumor and pharmacogenomic profiles of the patient into decision making.
Ethics Approval and Consent to Participate
The study was approved by the local ethics committee at the Kochi Health Sciences Center.
Consent for Publication
Written informed consent was obtained from the patients for publication of this case report and any accompanying images.
Competing Interests
The Authors declare that they have no competing interests
Acknowledgement
This work was supported by the Kochi organization for medical reformation and renewal grants.
References
- Modlin IM, Lye KD, Kidd M (2003) A 5-decade analysis of 13,715 carcinoid tumors. Cancer 97: 934-959.
- Yao JC, Hassan M, Phan A, Dagohoy C, Leary C, et al. (2008) One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 26: 3063-3072.
- Elias D, Lasser P, Ducreux M, Duvillard P, Ouellet JF, et al. (2003) Liver resection (and associated extrahepatic resections) for metastatic well-differentiated endocrine tumors: A 15-year single center prospective study. Surgery 133: 375-382.
- Mayo SC, De Jong MC, Pulitano C, Clary BM, Reddy SK, et al. (2010) Surgical management of hepatic neuroendocrine tumor metastasis: Results from an international multi-institutional analysis. Ann Surg Oncol 17: 3129–3136.
- Glazer ES, Tseng JF, Al-Refaie W, Solorzano CC, Liu P, et al. (2010) Long-term survival after surgical management of neuroendocrine hepatic metastases. HPB (Oxford). 12: 427-433.
- Saxena A, Chua TC, Sarkar A, Chu F, Liauw W, et al. (2011) Progression and survival results after radical hepatic metastasectomy of indolent advanced neuroendocrine neoplasms (NENs) supports an aggressive surgical approach. Surgery 149: 209-220.
- Chamberlain RS, Canes D, Brown KT, Saltz L, Jarnagin W, et al. (2000) Hepatic neuroendocrine metastases: does intervention alter outcomes? J Am Coll Surg 190: 432-445.
- Birnbaum DJ, Turrini O, Vigano L, Russolillo N, Autret A, et al. (2015) Surgical management of advanced pancreatic neuroendocrine tumors: Short-term and long-term results from an international multi-institutional study. Ann Surg Oncol 22: 1000-1007.
- Bosman FT, Carneiro F, Hruban RH, Theise ND (2010) WHO classiï¬ÂÂÂÂcation of tumours of the digestive system 3.
- Rizvi SM, Wong J, Saif MW, Jia Y (2014) Pharmacogenetics in neuroendocrine tumors of the pancreas. JOP 15: 299-302.
- Du S, Wang Z, Sang X, Lu X, Zheng Y, et al. (2015) Surgical resection improves the outcome of the patients with neuroendocrine tumor liver metastases: Large data from Asia. Medicine (Baltimore) 94: 388.
- Pavel M, Baudin E, Couvelard A, Krenning E, Öberg K, et al. (2012) Barcelona Consensus Conference participants. ENETS Consensus Guidelines for the management of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut, and unknown primary. Neuroendocrinology 95: 157-176.
- Rinke A, Müller HH, Schade-Brittinger C, Klose KJ, Barth P, et al. (2009) PROMID Study Group: Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the PROMID Study Group. J Clin Oncol 27: 4656-4663.
- Yao JC, Shah MH, Ito T, Bohas CL, Wolin EM, et al. (2011) Everolimus for advanced pancreatic neuroendocrine tumors. RAD001 in Advanced Neuroendocrine Tumors, Third Trial (RADIANT-3) Study Group. N Engl J Med 364: 514-523.

