Nabiha Khalid1, Zunaira Aslam1, Farzana Kausar2, Humayun Irshad3 and Pervez Anwar1,4*
1Department of Biochemistry and Molecular Biology, University of Gujrat, Sialkot, Pakistan
2Department of Biochemistry and Biotechnology, University of Gujrat, Pakistan
3Department of Chemistry, University of Gujrat, Sialkot, Pakistan
4Department of Bioinformatics and Biotechnology, International Islamic University, Islamabad, Pakistan
*Corresponding Author:
Anwer P
Department of Biochemistry and Molecular Biology
University of Gujrat, Sialkot, Pakistan
Tel: +0345-5480392
E-mail: pervez.anwer@uogsialkot.edu.pk
Received Date: December 15, 2017; Accepted Date: December 27, 2017; Published Date: December 29, 2017
Citation: Khalid N, Aslam Z, Kausar F, Irshad H, Anwer P (2017) Maternal Malnutrition and Its Kick on Child Growth: An Alarming Trim for Pakistan. J Food Nutr Popul Health Vol.1 No.3:24
Keywords
Maternal malnutrition; Micro-nutrient deficiencies; Infants; Supplementation
Introduction
Malnutrition is a state of over or under nutrition and its consequences on maternal and child health are very alarming. Maternal malnutrition is the prime cause of mortality and morbidity in children. In less developed countries like Pakistan, has received less attention on maternal nutrition. Nutritional status of mother is responsible for a healthy child, currently it needs to be evaluated to unmask the causes of maternal malnutrition in Pakistan [1].
Malnutrition affects overall mother and child health, survival, economic productivity of individuals and a healthy development and growth of a child. Malnutrition turn up, of lack of essential micro-nutrients include vitamins and minerals, their deficiency leads to serious problems during gestation period in mother and stunting in child after pregnancy [2].
Maternal malnutrition is a crucial contributor of low body mass index, anemia, micro-nutrient deficiencies and long term cognitive impairments in child [3]. According to National Survey of Pakistan 2011 it is reported that Pakistan has a high prevalence of child and mother under-nutrition. 44% children in Pakistan have stunted growth and one in two mothers is anemic due to lack of iron [4].
Micronutrients are collectively reported as vitamins and minerals. These micronutrients play essential role in the physiology of body their deficiency causes severe outcomes in maternal body and in fetus. Micronutrient deficiencies mostly reported in middle and low-income countries and cause several abnormalities like mental impairment [5]. Micronutrient deficiencies pose serious health effects on fetus and on mother such as irondeficiency anemia, pre-term births, post-partum hemorrhage, mental retardation, stunted growth of child are some of the outcomes of maternal malnutrition [6]. With the emerging motif of science and technology researchers find alternative approaches to overcome malnutrition in low-income countries. Oral supplements of vitamins and minerals are commercially available is one of the useful practice to deal with micronutrient deficiencies. Fortification and Bio-fortification of staple foods by plant breeding methods is also the egress in this biotechnology era [7].
Pakistan government has taken some initiatives and just started some nutrition programs with the collaboration of UNESCO and UN to control maternal malnutrition and child under-nutrition in Pakistan. Nutrition Intervention program has initiated by Khyber Pakhtunkhwa government to acknowledge public about nutritional supplements during pregnancy in pregnant females [8].
Malnutrition
Malnutrition is a condition of imperfect and inexact nutrition. It is of two types: over-nutrition and undernutrition, but scientists reported undernutrition and malnutrition synonymously because in the population of Asia undernutrition is more prevalent. In developing countries like Pakistan children and women are the two victims of malnutrition madly. The nutritional cachet of females is a key parameter for their healthy pregnancy. Undernutrition in women or maternal malnutrition is responsible for the poor fetal growth, fetus morbidity, fetus mortality and low body mass index. These impairments lead to the permanently lifetime defects in infants i.e., poor mental development [2]. In Pakistan, maternal malnutrition is higher in lactating and in pregnant females as compared to non-pregnant females [9].
Causes of malnutrition
Maternal malnutrition is unremitting cling in South Asian countries. Investigators has reported multifarious factors for the maternal malnutrition in developing countries i.e., lack education, poverty (Figure 1) and lack of empowerment are considered as dominant obstacles in malnutrition in women. Many women suffering from stresses and these include inadequate supply of food, chronic energy deficit and poor healthcare [9].
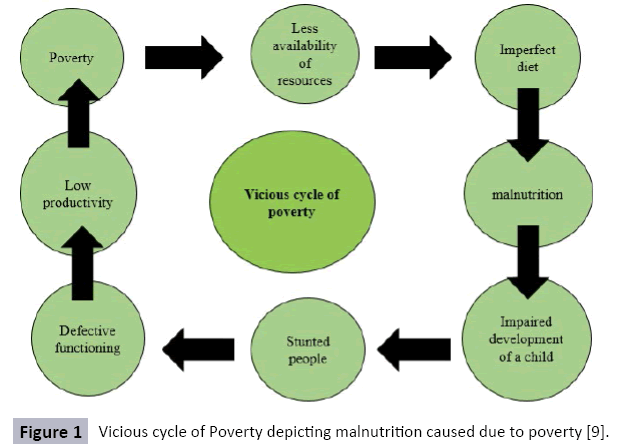
Figure 1: Vicious cycle of Poverty depicting malnutrition caused due to poverty [9].
According to recent study in Pakistan it is considered that there are most probable four reasons of malnutrition in Pakistan. In Pakistan with low income level poverty is considered a reason of malnutrition. Second reason revealed of malnutrition in a study is Breastfeeding, because well-nourished females have healthy pregnancies. Due to low food expenditures women have low productive lives and as a result low breastfeeding to their newborns. Low level of Breastfeeding affect child growth. According to World Health Organization (WHO) breastfeeding is the sole source of vitamins, minerals and essential nutrients to the young ones. Food insecurity is considered as a third key contributor in malnutrition in Pakistani society. Due to food crisis, globally food insecurity has become a threat in Pakistan. Despite this, natural disasters e.g., famines, floods have become the issues for food insecurity in Pakistan. In Sindh, Tharparkar districts have poor nutritional status due to less food availability has led to many deaths [10].
Micronutrient deficiencies
Micronutrient deficiencies can affect any age group but these are more rampant in women during their childbearing age. Iron deficiency anemia is one of the most prevalent and observed complication globally but the most affected victims of iron deficiency anemia are women of developing countries. The primary cause of anemia is iron but poor dietary habits, inadequate supply of nutrients, menstruation and nutritional demands of the fetus during gestation period are the more pronounced secondary causes of anemia in pregnant females. In Pakistan, the prevalence of iron-deficiency anemia in maternal population are varied i.e., in married females of age 15-44 is reported 26% in urban areas while females of rural areas have iron deficiency anemia is reported to be 47%. Similarly, the prevalence of anemia in pregnant females is reported 29%-55% in urban areas attending private clinical checkups in tertiary hospital in Karachi [11].
Study conducted in Rawalpindi at tertiary healthcare center to depict the deficiencies of iron, folate and cobalamin. It is reported that in pregnant females iron deficiency is about (57%), folate (20%) and cobalamin (4%) during their first trimester. In Pakistan, it is reported that deficiency of iron is due to poor reabsorption of iron due to intake of chapatti because chapatti contains phytates, an inhibitor of iron reabsorption [8]. Recently revealed that 70% of pregnant females have iron-deficiency anemia is due to the lack of vitamin B12 deficiency [12].
Vitamin A deficiency is also more pronounced deficiency in pregnant females in Pakistan. It is reported that children affected by measles have VAD which could be controlled by giving high doses of vitamin A. In Karachi, low serum retinol concentration is reported in pregnant females with night blindness detected [13].
Vitamin D is a steroid based vitamin and responsible for bone metabolism in body. During pregnancy vitamin D is most active in reproductive tissues and involved in immune modulation of body. Its deficiency causes severe effects on pregnant female and on its child, such as Preeclampsia, hypertension, gestational diabetes and preterm delivery and low birth weight of baby has been reported [14].
Women of low-income countries may develop hypothyroxinemia due to less dietary intake of iodine. In South Asian countries, Pakistan is thought-about the most iodine deficient country and the most prevalent cases have been reported in pregnant females. Due to iodine deficiency thyroid hormones not properly produce T3 levels in a body. This thyroid hormone is responsible for proper brain and neuronal development of fetus by the regulation of specific genes as a result fetus may abnormally developed nervous system [15].
Zinc plays imperative role in the production of cellular proteins, cellular division and in nucleic acid metabolism (Table 1). Zinc deficiency has stern effects on fetal health, one of the most reported effect due to zinc deficiency is feotal death due to abnormal production of proteins, impaired cellular division and in chromosomal defects. Zinc deficiency has some long-term effects on offspring such as immune dysfunction and on growth of the surviving offspring [16,17].
Table 1 Demonstration of required nutrients and their physiological effects in pregnant females and on foetus.
| Maternal nutritional requirements during pregnancy |
| |
Nutrients |
Dietary sources |
Nutritional value |
Deficiency outcomes |
References |
| Macronutrients |
Proteins |
Milk, beans and eggs |
Precursors for neurotransmitters, nitrogenous bases, signalling molecules and vasodilators |
Anaemia, maternal impaired blood flow, growth retardation of foetus and weakness |
[18] |
| Lipids |
Dairy products, oils and fats |
Development of foetus tissues, nervous system development, membrane permeability |
Impair foetus growth and development, maternal weight loss |
[18] |
| Carbohydrates |
Milk, vegetables, beans |
Basic energy currency, role in antioxidant reactions |
Maternal weight loss, fetal growth retardation and fatigue |
[19] |
| Vitamins |
Biotin
Vitamin B7 |
Fresh vegetables and meat |
Acts as co-enzyme A for ATP- dependent carboxylases, for the development of embryo |
Muscle pain, dermatitis in mother and depression |
[20] |
Folate
Vitamin B9 |
Fortified foods, leafy and green vegetables and legumes |
For nucleic acid synthesis and for constant cell division, spina bifida formation and skull development |
Defects in neural tube development (anencephaly in foetus) |
[20] |
Cobalamin
Vitamin B12 |
Meat |
For RBC’s production and nervous system development |
Anaemia, neurological disorders and cardiovascular complications |
[21] |
| Vitamin D |
Milk, de-novo synthesis by sunlight |
Required for calcium reabsorption, skeletal development of foetus |
Defective skeleton growth and rickets |
[22] |
| Vitamin A |
Milk, dark colour vegetables and fruits and eggs |
Required for vision, proper cellular differentiation, boosts immunity |
Maternal Night blindness, immune dysfunction of foetus |
[23] |
| Vitamin K |
Vegetables |
Bleeding when is cut occur |
Maternal haemorrhage |
[20] |
| |
Vitamin E |
Fresh fruits and vegetables, meat and animal fats |
Aid in Foetus RBC’s production |
Anaemia (may maternal or foetus) |
[20] |
| Vitamin C |
Fresh vegetables and fruits s |
Development of connective tissues of foetus |
Impaired collagen structure |
[20] |
| Minerals |
Iron |
fortified food products, meat and legumes |
RBC’s production |
Maternal or foetus iron-deficiency anaemia, maternal mortality or pre-term birth |
[18] |
| Iodine |
Sea-food, vegetables and iodised salt |
Myelination of neurons, neuronal migration and synaptic transmission during foetal development |
Cretinism (stunted mental growth) |
[24] |
| Zinc |
Legumes and meat |
Restricted fetal growth, regulation of food intake |
Malnutrition due to distracted regulation of food intake, immune dysfunction |
[18] |
| Calcium |
Milk and dairy products |
Bone development, cell signalling |
Pre-term births, pre-eclampsia and eclampsia |
[25] |
| Magnesium |
Meat |
Cofactor for different enzymatic reactions |
Pre-term delivery and pre-eclampsia |
[26] |
| Potassium |
Dairy product, meat and fresh vegetables |
Fetal development, maintains intracellular osmolality |
Cardiac arrest |
[20] |
Maternal malnutrition outcomes on maternal health
Malnourished women face different problems during their gestation period at different intervals which may leads severe dilemmas (Figure 2). Severe iron-deficiency anaemia during pregnancy is one of the most frequent complication observed in low-income [17-25]. Second major issue reported during pregnancy in malnourished females is postpartum haemorrhage. Each year 140,000 females dying due to postpartum haemorrhage. Primary issue of postpartum haemorrhage is the lack of uterine muscle contraction which may leads to frequent bleeding and it is known as uterine atony. This postpartum haemorrhage is the leading cause of mortality and morbidity in pregnant females in Pakistan as well as globally. Pre-eclampsia is considered as third contributing factor in maternal mortality in Pakistan. Pre-eclampsia is a condition linked with high blood pressure during pregnancy. According to Pakistan demographic and Health survey of 2007 reported that lack of MgSO4 use in low and middle-income countries is the leading cause of preeclampsia. These factors have high risk of maternal mortality and severe effects on child growth [6,26].
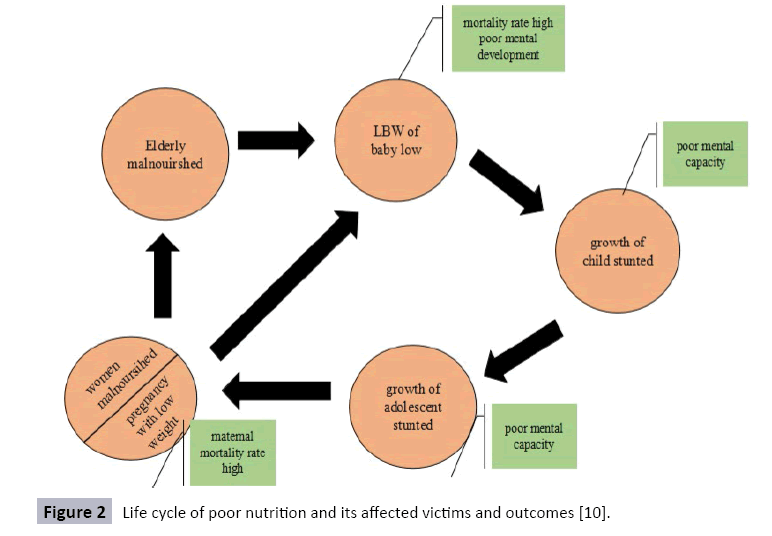
Figure 2: Life cycle of poor nutrition and its affected victims and outcomes [10].
Maternal malnourishment outcomes on infants
Iron deficiency in pregnant females may lead to low birth weight of their infants (Figure 2). Preterm births are the second more pronounced issue in Pakistan. It is reported that postpartum haemorrhage in pregnant females may often results in preterm births [27]. According to recent study it is reported that maternal stress and depression may the reason of preterm births. Biochemical mechanism of undernutrition is leads to the stress condition in pregnant female as a result cortisol releases from adrenal gland, this cortisol causes the release of oxytocin from posterior pituitary gland. In result, these hormones initiate the production of prostaglandins F2α (PGF2α) by the uterus, fetus and placenta. High levels of oxytocin bind with the intracellularly Gq type G-protein coupled receptors ultimately cause the release of second messengers Phospholipase C and Diacylglycerol via the inositol 1,4,5-trisphosphate pathway in turn, cause the in-flux of Ca+2 into the cell. This high level of Ca+2 causes the preterm contraction of the uterus ultimately cause pre-term births. On the other hand dietary supplementation consists of adequate amount of antioxidant micronutrients and omega-3 polyunsaturated fatty acids prevent preterm-birth (Figure 3) [28].
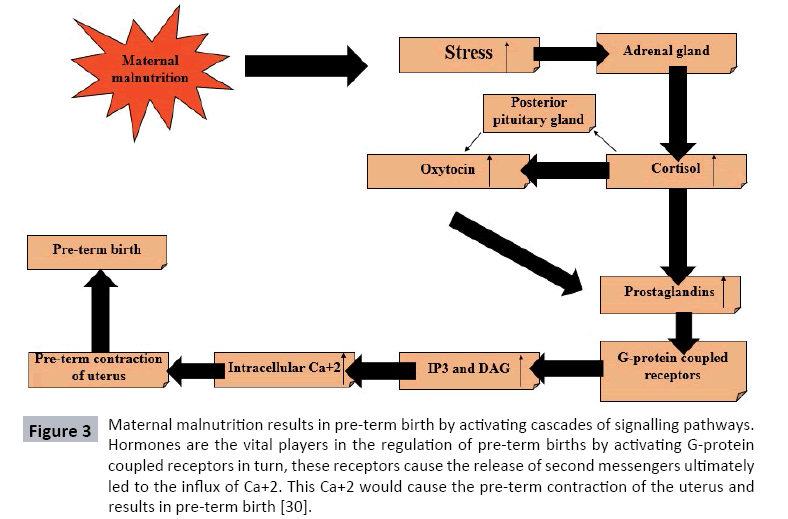
Figure 3: Maternal malnutrition results in pre-term birth by activating cascades of signalling pathways. Hormones are the vital players in the regulation of pre-term births by activating G-protein coupled receptors in turn, these receptors cause the release of second messengers ultimately led to the influx of Ca+2. This Ca+2 would cause the pre-term contraction of the uterus and results in pre-term birth [30].
Perinatal mortality is may also the maternal malnourishment consequence and health of a mother describes the health of her child. Intricacies or complications during pregnancy, delivery may often lead to the stillbirths or perinatal mortality. Maternal anaemia, diabetes and hepatitis are contributing factors in perinatal mortality. It is reported in a study conducted in Pakistan 270,000 new-borns die out of 5.3 million births [29]. Small for gestational age (SGA) is a state in which infants weight and size is less than the average size and weight of the infants of the same gestational age. SGA is not a key contributor in infant mortality but it has more pronounced effects in later adult life i.e., cardiovascular diseases and diabetes. Preeclampsia, stress and low or high BMI of mother are reported factors in SGA [30].
Strategies to overcome micro-nutrient deficiencies
Supplementation: Micronutrient supplementation is recommended to pregnant females for healthy pregnancy. These supplements have healthy impact on pregnant females and on fetus [31]. During pregnancy, folic acid supplementation is one of the best intervention for fetus growth and neural tube formation in fetus. Iron supplementation along with folic acid is necessary for the reduced risk of anemia in new-born as well as in mother. Oral iron supplementation is one of the alternative to prevent anemia [32]. Vitamin D supplementation is also the useful approach to enhance the responsiveness of neonate immune system. Vitamin D can activate different cytokines for inflammatory reactions [26]. Besides these micronutrients, oral supplements for zinc and iodine are also available [33].
Fortification: Fortification is the process of addition of micronutrients (vitamins and minerals) in a food. It is one of the propitious approach to fulfil the needs of micronutrients. Different fortification programs and has been designed in South Asia for adequate fortified intake of food. Fortified iron fish sauce designed to meet the demands of iron by the Reproductive and Child Health Alliance (RACHA) with the collaboration of National Sub-committee for Food Fortification [34]. Studies suggested that food fortification with iron, folate, vitamin D and A, zinc and iodine is one of the most common fortification practices for women and children [7].
Bio-fortification: With the emerging science biofortification become the most useful and appropriate tool to reduce micronutrient deficiencies globally. Biofortification is a method to enhance the nutritional quality of staple food by biotechnology approaches, through transgenic techniques or by plant breeding methods. Plant breeders increase the micronutrient level in the food crops to meet the demand of micronutrients by plant breeding method as a result biofortified foods obtained [35].
Pakistan government initiatives to control malnutrition in Pakistan
Tawana Pakistan Project is one of the initiative by the government of Pakistan with the collaboration of Ministry of social welfare to convoy young girls and women to run nutritional awareness. With this program, almost 94,000 women were trained to combat malnutrition. With this initiative, a clear drop seen in malnutrition and in stunting in girls of primary schools.
Micronutrient initiative program designed with the aid of UN to eliminate micronutrient deficiencies among people of Pakistan. MI program screened micronutrient deficiencies among people of different target areas and provide them to proper supplementation of zinc and vitamin A, folic acid. Family planning and primary Healthcare program is another initiative of government to acknowledge people with the primary health care provided by the lady health workers especially in rural areas. The area of focus of this program is to provide sufficient information about maternal malnutrition and child health [36].
Nutritional intervention program started by the government of North West Pakistan to increase knowledge of nutritional supplements during pregnancy, importance of breastfeeding to infants. This program involved the local community and lady health workers for acknowledging mothers for nutritional supplements and in the design of nutritional status for mothers and infants [8].
Conclusion
Malnutrition has become a global issue and it contributes key problems in a population of Pakistan especially targeting women and children. Malnourishment is totally linked with the mortality and morbidity in females and in children. Malnutrition in females results still births, post-partum hemorrhage and pre-term births. This would lead to the stunted growth in children and cognitive impairments and poor development. This stunting and wasting of children due to malnourishment become a hurdle in a national progress and would not be able as much productive. Pakistan government has made policies and initiate some nutritional related health program to control malnutrition in women and children of Pakistan.
References
- Saeed Q, Shah N,Inam S, Shafique K (2017) Maternal depressive symptoms and child nutritional status: A cross-sectional study in socially disadvantaged Pakistani community. Journal of Child Health Care 21: 331-342.
- Black RE,Victora CG,Walker SP, Bhutta ZA, Christian P, et al. (2013) Maternal and child undernutrition and overweight in low-income and middle-income countries. The Lancet 382: 427-451.
- Imdad A, Bhutta ZA (2012) Maternal nutrition and birth outcomes: Effect of balanced proteinâ€ÂÂÂÂenergy supplementation. Paediatric and Perinatal Epidemiology 26: 178-190.
- Khan DA, Fatima S, Imran R, Khan FA (2010) Iron, folate and cobalamin deficiency in anaemic pregnant females in tertiary care centre at Rawalpindi.J Ayub Med Coll Abbottabad 22: 17-21.
- Black R (2003) Micronutrient deficiency: an underlying cause of morbidity and mortality. Bulletin of the World Health Organization 81: 79.
- Edhi MM, Aslam HM, Naqvi Z, Hashmi H (2013) Post partum hemorrhage: causes and management. BMC Research Notes 6: 236.
- Das JK, Salam RA, Kumar R, Bhutta ZA (2013) Micronutrient fortification of food and its impact on woman and child health: a systematic review. Systematic Reviews 2: 67.
- Lhussier M, Bangash S, Dykes F, Zaman M, Lowe NM (2011) Development and implementation of a nutrition intervention programme in North West Pakistan: a realist framework. Health promotion international 27:453-462.
- Ahmed T (2012) Global burden of maternal and child undernutrition and micronutrient deficiencies. Annals of Nutrition and Metabolism 61:8-17.
- Zulfiqar Z, Ghazanfar S, Shahzadi S,Mehmood MK (2017) Causes and Consequences of Malnutrition. The Explorer Islamabad: Journal of Social Sciences 2: 38-42.
- Baig-Ansari N, Badruddin SH, Karmaliani R, Harris H, Jehan I, et al. (2008) Anemia prevalence and risk factors in pregnant women in an urban area of Pakistan.Food and Nutrition Bulletin 29: 132-139.
- Noronha JA, Khasawneh SA, Seshan V, Ramasubramaniam S, Raman S(2012) Anemia in pregnancy-consequences and challenges: a review of literature. Journal of South Asian Federation of Obstetrics and Gynecology 4: 64-70.
- Akhtar S,Ahmed A, Randhawa MA, Atukorala S, Arlappa N, et al. (2013) Prevalence of vitamin A deficiency in South Asia: causes, outcomes, and possible remedies. J Health PopulNutr 31: 413-423.
- Urrutia RP, Thorp JM (2012) Vitamin D in pregnancy: current concepts. Current Opinion in Obstetrics &Gynecology 24: 57-64.
- Elahi S, NagraSA (2014) Low maternal iodine intake and early pregnancy hypothyroxinemia: Possible repercussions for children. Indian Journal of Endocrinology and Metabolism 18: 526-530.
- Chaffee BW, King JC (2012) Effect of zinc supplementation on pregnancy and infant outcomes: a systematic review. Paediatric and Perinatal Epidemiology 26: 118-137.
- Kalhan SC, D'Angelo LJ, Savin SM, Adam PAJ(1979) Glucose production in pregnant women at term gestation: Sources of glucose for human fetus. Journal of Clinical Investigation 63: 388-394.
- Wu G, Imhoff-Kunsch B, Girard AW (2012) Biological mechanisms for nutritional regulation of maternal health and fetal development. Paediatric and Perinatal Epidemiology 26: 4-26.
- Allen LH (1994) Vitamin B12 metabolism and status during pregnancy, lactation and infancy. Nutrient Regulation during Pregnancy, Lactation, and Infant Growth Springer: 173-118.
- Zehnder D, Evans KN,Kilby MD, Bulmer JN, Innes BA, et al.(2002) The ontogeny of 25-hydroxyvitamin D(3) 1α-hydroxylase expression in human placenta and decidua. The American Journal of Pathology 161: 105-114.
- Rothman KJ, Moore LL, Singer MR, Nguyen UDT, Mannino S, et al. (1995) Teratogenicity of high vitamin A intake. New England Journal of Medicine 333: 1369-1373.
- Lewandowski TA, Peterson MK, Charnley G (2015) Iodine supplementation and drinking-water perchlorate mitigation. Food and Chemical Toxicology 80: 261-270.
- Imdad A, BhuttaZA (2012) Effects of calcium supplementation during pregnancy on maternal, fetal and birth outcomes. Paediatric and Perinatal Epidemiology 26: 138-152.
- 24.Romani AM (2011) Cellular magnesium homeostasis. Archives of biochemistry and biophysics 512: 1-23.
- 25.Imdad A,Bhutta ZA (2012) Routine iron/folate supplementation during pregnancy: effect on maternal anaemia and birth outcomes. Paediatric and Perinatal Epidemiology 26: 168-177.
- Bigdeli M, Zafar S, Assad H, Ghaffar A (2013) Health system barriers to access and use of magnesium sulfate for women with severe pre-eclampsia and eclampsia in Pakistan: evidence for policy and practice. PloS One 8: e59158.
- Shaikh K,Premji SS, Rose MS, Kazi A, Khowaja S, et al. (2011) The association between parity, infant gender, higher level of paternal education and preterm birth in Pakistan: a cohort study. BMC Pregnancy and Childbirth 11: 88.
- Neumann ID (2002) Involvement of the brain oxytocin system in stress coping: interactions with the hypothalamo-pituitary-adrenal axis.Progress in Brain Research 139: 147-162.
- Iqbal M, Majid A, Muhammad Z, Khan HA (2014) Perinatal mortality and its related obstetrics risk factors.J Med Sci 22: 76-79.
- Ota E,Ganchimeg T, Morisaki N, Vogel JP, Pileggi C, et al. (2014) Risk factors and adverse perinatal outcomes among term and preterm infants born small-for-gestational-age: secondary analyses of the WHO Multi-Country Survey on Maternal and Newborn Health. PLoS One 9: e105155.
- Haider BA,Bhutta ZA (2012) Multiple-micronutrient supplementation for women during pregnancy. Cochrane Database Syst Rev 11: CD004905.
- Peñaâ€ÂÂÂÂRosas JP, De-Regil LM, Garcia-Casal MN, Dowswell T (2012) Daily oral iron supplementation during pregnancy.The Cochrane Library 7: CD004736.
- Zehnder D, Evans KN, Kilby MD, Bulmer JN, Innes BA, et al. (2002) The ontogeny of 25-hydroxyvitamin D 3 1α-hydroxylase expression in human placenta and decidua. The American journal of pathology 161: 105-114.
- Gayer J, Smith G (2015) Micronutrient fortification of food in Southeast Asia: recommendations from an expert workshop. Nutrients 7: 646-658.
- Bouis HE, Welch RM (2010) Biofortification-a sustainable agricultural strategy for reducing micronutrient malnutrition in the global south. Crop Science 50: S-20-S-32.
- Niazi AK,Niazi SK, Baber A (2012) Nutritional programmes in Pakistan: a review. Journal of Medical Nutrition and Nutraceuticals 1: 98.