Keywords
Lymphocyte-to-monocyte ratio; Melatonin; Metoxytryptamine; Pineal gland
Introduction
Each living organisms may generate both pro-tumoral and anti-tumoral events, from whose equilibrium depends the physiological growth of the normal cells until their apoptosisinduced death. The antitumor biological response, which is responsible for the natural resistance against cancer growth, would depend not only on immune factors, but also on the physiological psychoneuroendocrine regulation of the immune system, which may act by either stimulating or suppressing the antitumor immunity, as shown by the great number of researches in the area of the Psycho-neuro-endocrinoimmunology (PNEI) [1-3]. In particular, it has been shown that the opioid system may inhibit the anticancer immunity [4] by promoting the generation of regulatory T lymphocytes (T reg), which may suppress the antitumor immune response through the secretion of immunosuppressive cytokines, such as TGFbeta and IL-10 [5], and by inhibiting T helper-1 lymphocyte (TH1) and dendritic cells functions [6], with a following decline in the production of IL-2 and IL-12, respectively, that represent the main antitumor cytokines in humans [7,8]. On the contrary, the anticancer immunity has been proven to be stimulated by the pineal gland through the release of several indole hormones [9] and beta-carbolines [10], whose activity is connected with the brain cannabinergic system, by constituting a fundamental neuroendocrine functional axis [11]. More in detail, stress-induced promoting effect on cancer onset and development has appeared to be mediated by the opioid system, mainly through the release of mu-opioid agonists, such as the beta-endorphin, since it may be blocked by the concomitant administration of the mu-opoid antagonist naltrexone [4]. On the other hand, pleasure and spiritual expansion of mind may counteract tumor dissemination by activating the pineal-cannabinergic functional axis [12]. As far as the pineal activity is concerned, the main anticancer molecules are consisting of the indoles melatonin (MLT) and 5- methoxytryptamine (5-MTT) [9], and the beta-carboline pinealine [10], which exert their anticancer action by either directly inhibiting cancer cell proliferation, or stimulating the anticancer immunity, namely through the activation of TH1 lymphocytes and dendritic cells, with a following enhanced production of IL-2 and IL-12 [13,14]. The antitumor immunomodulating effects of MLT are mainly due to the stimulation of lymphocyte functions [15], whereas those played by 5-MTT, pinealine, as well as by cannabinoids, would mainly depend on an inhibition of macrophage-mediated immuno-inflammatory response [9,10], which has been proven to suppress the anticancer immunity [16,17]. Therefore, from a neuroimmune point is concerned, cancer growth may be considered as the consequence of an altered balance involving the main structures responsible for the neuroimmunomodulation of the immune responses, consisting of an enhanced brain opioid sistem activity in association with a concomitant diminished function of the pineal-cannabinergic system axis [18]. In fact, the progressive decline in the pineal function, namely consisting of a progressive lack of the nocturnal increase in MLT levels with a consequent disappearance of its physiological light/dark circadian rhythm [19], would represent the main cancer progression-related endocrine deficiency either in animals, or in humans [20,21]. Cancer-related pineal endocrine deficiency woul regard not only MLT, but probably the whole pineal endocrine activity, since pineal histological damages have been described in patients died from cancer [22]. However, despite it is known since more than 50 years that the pineal gland plays a fundamental role in the maintenance of the natural anticancer immunobiological resistance [9-11] and the complete absence of any biological toxicity exerted by the pineal indole and beta-carboline hormones [19], few clinical studies have been performed up to now with MLT alone or MLT in association with other antitumor pineal molecules to evaluate their efficacy in the treatment of advanced cancer patients, who failed to respond to the conventional chemotherapies and target therapies, at least in terms of palliative therapy. In any case, preliminary clinical studies have already shown that high-dose MLT alone may induced a stabilization of the neoplastic disease in a clinically relevant percentage of cancer patients, for whom no other standard anticancer therapy was available, and with life expectancy less than 6 months-1 year [23]. Moreover, it has been shown that the anticancer activity of MLT is a dose-dependent phenomenon, and may be further amplified by the concomitant administration of other antitumor pineal molecules, namely 5-MTT and pinealine [23-25]. However, many others natural anticancer strategies have been elaborated in the last year [26-28]. The present study reports the 5-year survival achieved by the pineal endocrine therapy with high-dose MLT plus 5-MTT plus pinealine in advanced cancer patients, for whom no other standard antitumor therapy was available, and its relation with the clinical response and the immune status by determining the lymphocyte-to-monocyte ratio (LMR), which has been proven to reflect and to synthetize the complex interaction between immunosuppressive and immunostimulatory events involved in the antitumor immunity [29].
Materials and Methods
Patient enrollment
The study included 212 advanced cancer patients, for whom no other standard anticancer therapy was available, then eligible for the only palliative treatment, who had a follow up of at least five years. Eligibility criteria were, as follows: histologically proven solid tumor, measurable lesions, metastatic or advanced neoplastic disease, no availability of conventional anticancer therapy because of lack of response to the previous standard treatments or poor clinical conditions unable to sustain a chemotherapeutic approach, no double tumor, and life expectancy less than 1 year.
Study plan
All pineal hormones were given orally. MLT was administered at 100 mg/day during the dark period of the day, according to its physiological circadian rhythm, generally halfhour before sleeping. 5-MTT was given at 10 mg/day during the light phase of the day, generally at 1.00 P.M. Finally, pinealine was administered at 1 mg/day in the evening, generally 3 hours prior to sleep. Moreover, the supportive care was planned according to a phythotherapeutic approach, by using plants, which have been proven to give some subjective benefits in previous clinical studies [30], namely Aloe, Myrrh, and Magnolia. The treatment with pineal hormones was continued without interruption until disease progression. In the presence of a clear subjective clinical benefit, pineal hormone therapy was still continued despite the progression of the neoplastic disease. The clinical characteristics of patients are reported in Table 1. The clinical response was evaluated according to WHO criteria by repeating the radiological investigations, including CT scan and NMR, before the onset of treatments and at 3-month intervals until disease progression. Moreover, the clinical response was correlated with LMR values, which were detected prior to therapy and at 1-month intervals. Normal values of LMR obtained in our laboratory (95% confidence limits) were greater than 2.1. Data were statistically analyzed by the chi-square test, the Student’s t test. Finally, the survival curves were made according to the Kaplan-Meyer method, and statistically assessed by the logrank test.
Table 1 Characteristics of 212 untreatable advanced cancer patients treated with pineal endocrine therapy (PET).
| Characteristics |
n |
| M/F |
118/94 |
| Median age (years) |
63 (22- 92) |
| Median performance status 1 |
( 0 – 3) |
| Previous chemotherapy |
178/212 (84%) |
Results
Clinical response to therapy
The clinical response and the 5-year percentages of survival observed in the overall patients and in relation to the single tumor histotypes are reported in Table 2. A complete response (CR) was achieved in 2/212 (1%) patients (non-small cell lung cancer: 1; gastric cancer: 1). Moreover, a partial response (PR) was obtained in other 14/212 (7%) patients (non-small cell lung cancer (NSCLC): 2; colorectal cancer: 2; pancreatic adenocarcinoma: 1; hepatocarcinoma: 1; biliary tract cancer: 2; ovarian cancer: 2; bladder cancer: 1; triple negative breast cancer (TNBC): 1; melanoma: 2). Then, an objective tumor regression was achieved in 16/212 (8%) patients. A stable disease (SD) was observed in 95/212 (45%). Therefore, a disease control (DC) (CR+PR+SD) was achieved in 111/212 (52%) patients, whereas the remaining 101 patients (48%) had a progressive disease (PD). As shown, the 5-year survival observed in the overall patients and in relation to their clinical response is illustrated in Figure 1. The 1-year, 3-year and 5- year survival percentages were 46%, 18%, and 11%, respectively. Moreover, the survival time obtained in patients, who achieved an objective tumor regression (CR+PR), was significantly longer with respect to that found in those, who had no tumor regression (P<0.01). Finally, the survival time found in patients with SD was also significantly longer than that observed in patients with PD (P<0.05).
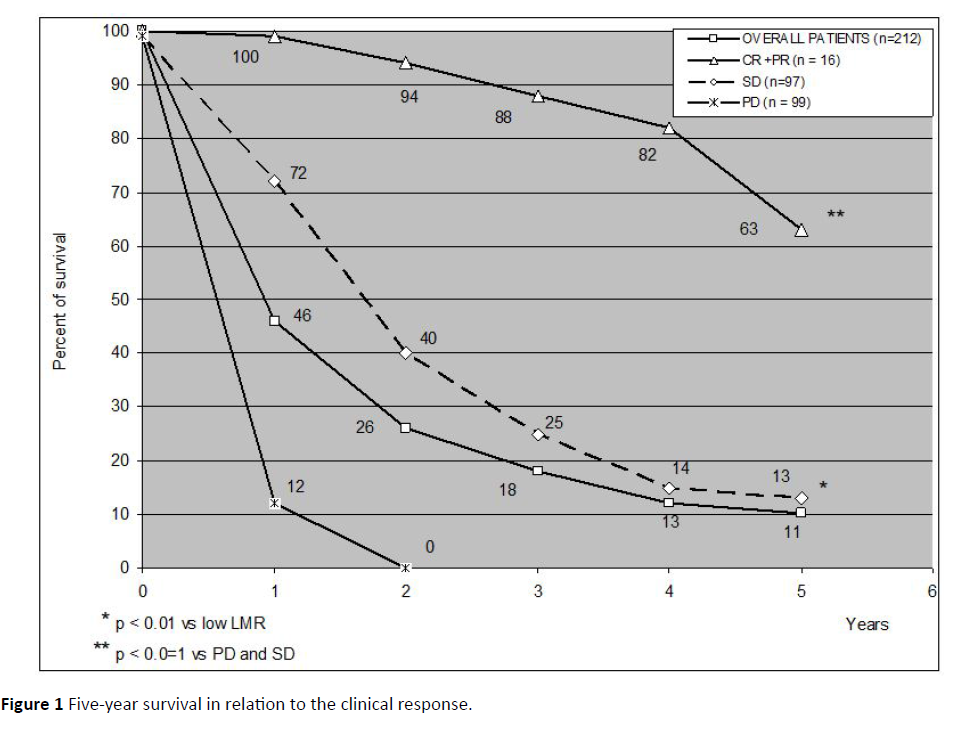
Figure 1: Five-year survival in relation to the clinical response.
Table 2 Clinical response (WHO citeria) and survival time to pineal endocrine therapy (P.E.T.) in 212 untreatable advanced cancer patients, and their relation to tumor histotype.
| Patients + |
Clinical Response ++ |
Survival Time (Year) |
| n |
CR |
PR |
CR + PR (%) |
SD |
DC (%) |
PD |
1 |
2 |
3 |
4 |
5 |
| Overall Patients |
212 |
2 |
14 |
16 (-8%) |
95 |
111 (-52%) |
101 |
98 (-46%) |
56 |
38 |
27 |
23 (-11%) |
| Tumor Histotype |
| Lung cancer |
36 |
1 |
2 |
3 |
16 |
19 |
17 |
17 |
9 |
7 |
5 |
5 |
| -NSCLC |
29 |
1 |
2 |
3 |
14 |
17 |
12 |
15 |
7 |
6 |
4 |
4 |
| -SCLC |
7 |
0 |
0 |
0 |
2 |
2 |
5 |
2 |
2 |
1 |
1 |
1 |
| Colorectal cancer |
25 |
0 |
2 |
2 |
13 |
15 |
10 |
13 |
8 |
5 |
4 |
4 |
| Pancreatic cancer |
22 |
0 |
1 |
1 |
10 |
11 |
11 |
12 |
4 |
3 |
2 |
1 |
| Gastric cancer |
12 |
1 |
0 |
1 |
3 |
4 |
8 |
3 |
3 |
3 |
2 |
1 |
| Biliary tract cancer |
11 |
0 |
2 |
2 |
2 |
4 |
7 |
6 |
3 |
2 |
2 |
1 |
| Hepatocarcinoma |
6 |
0 |
1 |
1 |
3 |
4 |
2 |
3 |
2 |
1 |
0 |
0 |
| Ovarian cancer |
14 |
0 |
2 |
2 |
7 |
9 |
5 |
9 |
6 |
3 |
2 |
2 |
| Bladder cancer |
5 |
0 |
1 |
1 |
3 |
4 |
1 |
3 |
2 |
1 |
1 |
1 |
| Prostate cancer |
4 |
0 |
0 |
0 |
3 |
3 |
1 |
3 |
3 |
2 |
2 |
2 |
| TNBC |
6 |
0 |
1 |
1 |
2 |
3 |
3 |
3 |
2 |
2 |
1 |
1 |
| Soft tissue sarcoma |
15 |
0 |
0 |
0 |
8 |
8 |
7 |
5 |
3 |
3 |
2 |
2 |
| Melanoma |
10 |
0 |
2 |
2 |
4 |
6 |
4 |
4 |
2 |
2 |
1 |
1 |
| Glioblastoma |
46 |
0 |
0 |
0 |
21 |
21 |
25 |
19 |
9 |
4 |
3 |
2 |
NSCLC: non-small cell lung cancer; SCLC: small cell lung cancer; TNBC: triple negative breast cancer, CR: complete response; PR: partial response; SD: stable disease; DC: disease control; PD: progressive disease
Immune effect of therapy
From the point of view of the immunological status is concerned, abnormally low pretreatments values of LMR were seen in 131/212 (62%) patients. The clinical response in relation to LMR pretreatment values are shown in Table 3. As reported, both objective tumor regression and DC percentages observed in patients with normal pretreatment values of LMR were significantly higher than those found in patients with abnormally low LMR values prior to therapy (P<0.01 and P<0.05, respectively). In addition, as illustrated in Figure 2, the 5-year percentage of survival observed in patients with normal LMR values prior to therapy was significantly longer than that achieved in patients with low pretreatment LMR values (P<0.01). Finally, as far as patients with PD are concerned, 44/101 (44%) patients, who had a PD, continued the pineal therapy despite the progression of their disease, because their improved clinical status. After 6 months and 1 year, only 34/ 101 (34%) and 2/101 (2%) were still alive. Both patients still alive at 1 year had continued the pineal therapy, whereas no patient, who interrupted the treatment, was alive. Moreover, the percentage of 9-month survival achieved in progressed patients, who continued the pineal therapy, was significantly longer than that found in those, who interrupted the endocrine treatment (14/44 (32%) vs. 0/57, P<0.05). Finally, abnormally low LMR values prior to therapy were seen in 70/101 (69%) patients with PD. The 9-month survival percentage observed in patients with PD but normal pretreatment values of LMR was significantly longer than that found in progressed patients with abnormally low values of LMR prior to therapy (9/31 (29%) vs. 5/70 (7%), P<0.05). The treatment was well tolerated, and most patients experienced a clear subjective benefit in mood, anxiety, sleep quality and asthenia. No biological toxicity occurred under pineal therapy, and some transient undesirable effects, such as headache, increase in anxiety, and sleep disturbances, occurred for few days in only 23/212 (11%) patients, without the need to interrupt the treatment.
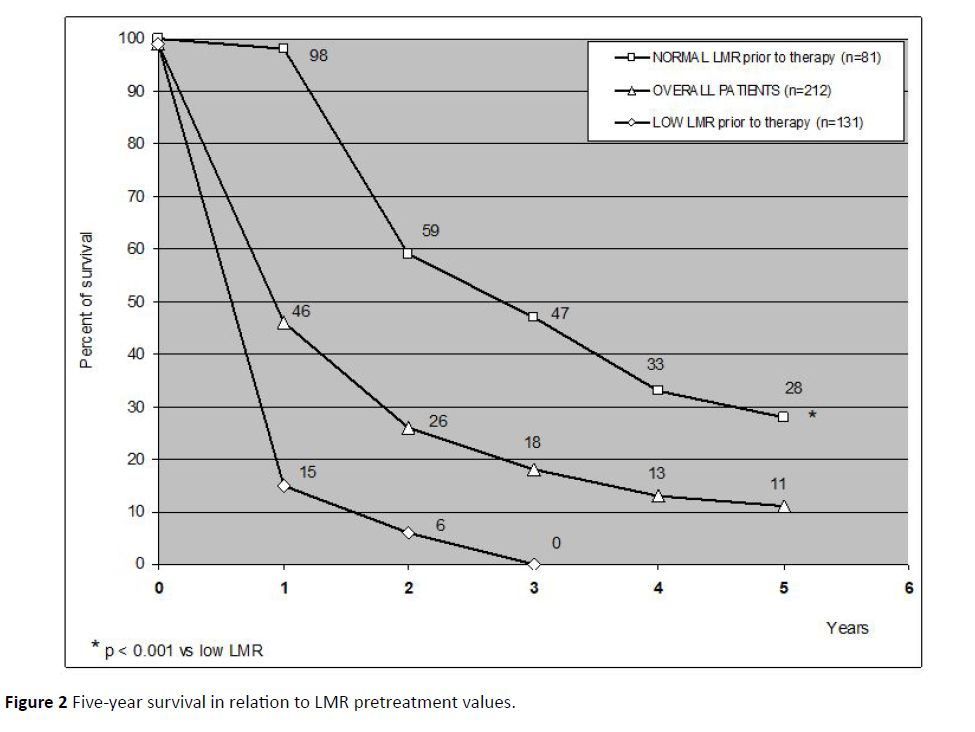
Figure 2: Five-year survival in relation to LMR pretreatment values.
Table 3 Clinical response (WHO criteria) in relation to LMR pretreatment values to pineal endocrine therapy (P.E.T.) in 212 untreatable advanced cancer patients.
| Lmr Pretreatment Values + |
Clinical Response ++ |
| n |
CR |
PR |
CR+PR (%) |
SD |
DC (%) |
PD (%) |
| Normal Values |
81 |
2 |
9 |
11 (14%) * |
52 |
63 (78%)** |
18 (22%) |
| Low Values |
131 |
0 |
5 |
5 ( 4%) |
43 |
48 (37%) |
83 (63%) |
+ LMR: lymphocyte-to-monocyte ratio; normal values more than 2.1; ++ CR: complete response; PR: partial response; SD: stable disease; DC: disease control; PD: progressive disease
*P<0.01 vs. low LMR values; P<0.05 vs. low LMR values
Discussion
According to previous preliminary clinical results [23-25], this study confirms in a greater number of untreatable advanced cancer patients and for a longer period of follow-up that the endocrine therapy with high-dose of MLT in association with the administration of the other two main anticancer molecules of the pineal gland, including 5-MTT and pinealine, may induce some tumor regression and prolong the survival time in patients eligible for the only palliative therapy because of the lack of response to the previous antitumor therapies, and life expectancy lower than 1 year. Moreover, the pineal endocrine therapy-induced prolongation of the survival time has appeared to be greater in patients, who achieved an objective tumor regression or disease stabilization, by suggesting that pineal endocrine-induced control of cancer growth is not a simple epiphenomenon, since it has been proven to predict a longer survival. This finding is not surprising since the only MLT has been already observed to represent the only molecule capable of counteracting the whole six main mechanisms responsible for cancer dissemination [23], including stress-induced immunosuppression, cancer cell transformation, intercellular joint alterations, stimulation of the neoangiogenic processes, tumor cell production of immunosuppressive factors and tumor expression of FAS-L, which allows the apoptosis of T lymphocytes after their interaction with the cancer cells [30]. In addition, the antitumor activity of MLT may be enhanced by the concomitant association with other pineal anticancer molecules, by justifying the possible evidence of tumor regressions or tumor stabilization also in very advanced cancer patients, for whom no other standard anticancer therapy may be available. Moreover, this study would suggest that the efficacy of a pineal endocrine antitumor therapy is greater in patients with normal pretreatment values of LMR, which may synthetize the whole status of the anticancer immunity in the single cancer patient [29]. The different efficacy of therapy may be influenced by the previous therapies, namely radiotherapy, because of the influence on lymphocyte count. Then, the evidence of abnormally low LMR values would reflect an immunosuppressive status of the anticancer immunity, with a consequent lower efficacy of the various anticancer treatments. Finally, previous studies had already shown a greater efficacy of the anticancer therapies in the presence of a real spiritual faith condition, as assessed by an adequate clinical test [31]. Some recent biomarkers, such as LMR, could be use full to clinically monitor the immune status of cancer patients [32,33]. Then, in the presence of a clinical response consisting of objective tumor regression or neoplastic disease stabilization, of a normal LMR values prior to therapy and an adequate spiritual faith score, it is probable that the pineal endocrine antitumor therapy may contribute to the control of the neoplastic growth and modify the prognosis of an untreatable advanced neoplastic disease also in patients, for whom no other conventional anticancer therapy may be available. On the contrary, tumor histotype does not seem to influence the efficacy of the pineal anticancer therapy in a relevant manner, even though glioblastoma and pancreatic adenocarcinoma would seem to represent the less responsible neoplasms to the treatment. However, by considering their low life expectancy after failure of the various therapies, glioblastoma and cancer of pancreas would be also influenced by the pineal therapy, at least in terms of survival time with respect to the expected one. Obviously, further randomized studies with the only best supportive care (BSC) or with BSC plus the pineal endocrine anticancer therapy will be required to confirm that the administration of the main anticancer molecules produced by the pineal gland may prolong the survival time also in patients with advanced cancer, eligible for the only palliative therapy and with life expectancy less than 1 year, since the survival of untreatable cancer patients, for whom no other standard anticancer therapy is available, is constantly generally less than 1 year or 6 months.
Conclusion
This preliminary study, by showing a possible increase in the survival time in patients with untreatable tumors and life expectancy less than 1 year, then suitable for the only supportive care by the simple administration of the immunostimulating pineal hormones would suggest that the separation between palliative and curative has to be abrogated by the existence in the nature of several non-toxic anticancer agents, namely within the same human body, which could be administered to untreatable cancer patients with respect to the only palliative therapy. Moreover, further studies by evaluating other immune parameters, such as tumor infiltrating lymphocytes, will be required to better define the immunomodulating effects of pineal therapy.
References
- Riley V (1981) Psychoneuroendocrine Influences On Immunocompetence And Neoplasia. Science 212: 1100-1109.
- Rubinow DR (1990) Brain, Behaviour and Immunity: An Interactive System. J Natl Cancer Inst Monoghr 10: 79-82.
- Antony MH (2003) Psychoneuroimmunology of Cancer. Brain Beav Immun 17: 84-91.
- Manfredi B, Sacerdote P, Pianchi M (1993) Evidence For An Opioid Inhibitory Tone On T Cell Proliferation. J Neuroimmunol 44: 43-46.
- Zou W (2006) Regulatory T Cells, Tumor Immunity And Immunotherapy. Nat Rev Immunol 6: 295-307.
- Antony PA, Restito NP (2005) CD4+CD25+ T Regulatory Cells, Immunotherapy Of Cancer And Interleukin-2. J Immunother 28: 120-128.
- Grimm EA, Mazumder A, Zhang HZ, Rosenberg SA (1982) Lymphokine-Activated Killer Cell Phenomenon. J Exp Med 155: 1823-1841.
- Banks RE, Patel PM, Selby PJ (1995) Interleukin-12: A New Clinical Player in Cytokin Therapy. Br J Cancer 71: 655-659.
- Sze SF, Ng TB, Liu WK (1993) Antiproliferative Effect of Pineal Indoles on Cultured Tumor Cell Lines. J Pineal Res 14: 27-33.
- Song Y, Wang J, Teng SF, Kesuma D, Deng Y, et al. (2002) Beta-Carbolines As Specific Inhbitors of Cyclin-Dependent Kinases. Biorg Med Chem Lett 12: 1129-1132.
- Lissoni P, Resentini M, Mauri R, Esposti D, Esposti G, et al. (1986) Effects Of Tetrahydrocannabinol On Melatonin Secretion In Man. Horm Metabol Res 18: 77-78.
- Grotenhermen F (2004) Pharmacology of Cannabinoids. Neuroendocrinol Lett 25: 14-23.
- Regelson W, Pierpaoli WM (1987) A Rediscovered Antitumor Hormone? Cancer Invest 5: 379-385.
- Guerrero JM, Reiter RJ (2002) Melatonin-Immune System Relationships. Curr Topics Med Chem 2: 167-180.
- Conti A, Maestroni GJM (1995) The Clinical Neuroimmunotherapeutic Role Of Melatonin In Oncology. J Pineal Res 19: 103-110.
- Mantovani A, Allavena P, Sica A, Balkwill F (2008) Cancer-Relòated Inflammatioopn. Nature 454: 436-444.
- Grivennikov SI, Greten FR, Karin M (2010) Immunity, Inflammation, And Cancer. Cell 295: 883-899.
- Lissoni P (2000) Is There A Role For Melatonin In Supportive Care? Supp Care Cancer 10: 110-116.
- Bartsch C, Bartsch H (1999) Melatonin in Cancer Patients And In Tumor-Bearing Aninals. Adv Exp Med Biol 467: 247-264.
- Brzezinski A (1997) Melatonin In Humans. N Engl J Med 336: 186-195.
- Lissoni P (1999) The Pineal Gland as A Central Regulator Of Cytokine Network. Neuroendocrinol Lett 20: 343, 349.
- Hadjiu SI, Porro RS, Lieberman PH (1972) Degeneration Of The Pineal Gland Of Patients With Cancer. Cancer 29: 706-709.
- Reiter RJ (2004) Mechanisms of Cancer Inhibition By Melatonin. J Pineal Res 37: 213-214.
- Millis E, Wu P, Seely D, Guyatt G (2005) Melatonin In the Treatment of Cancer: A Systematic Review Of Randomized Controlled Trials And Meta-Analysis. J Pineal Res 39: 360-366.
- Lissoni P, Messina G, Lissoni A, Rovelli F (2017) The Psychoneuroendocrine-Immunotherapy Of Cancer: Historical Evolution And Clinical Results. J Res Med Sci 22: 45-52.
- Wakaskar RRJ (2018) Brief Overview Of Nanoparticulate Therapy In Cancer. J Drug Target 26: 123-126.
- Wakaskar RRJ (2017) Passive And Active Targeting In Tumor Microenvironment. Int J Drug Dev & Res 9: 2.
- Wakaskar RRJ (2018) Promising Effects of Nanomedicine in Cancer Drug Delivery. J Drug Target 26: 319-324.
- Nishijma TF, Muss HB, Shachar SS, Tamura K, Takamatsu Y (2015) Prognostic Value Of Lymphocyte-To-Monocyte Ratio In Patients With Solid Tumors: A Systematic Review And Meta-Analysis. Cancer Treat Rev 41: 971-978.
- Shibakita M, Tachibana M, Dhar DK, Kotoh T, Kinugasa S, et al. (1999) Prognostic Signififance Of FAS And FAS Ligand Expression In Human Esophageal Cancer. Clin Cancer Res 5: 2464-2469.
- Messina G, Rovelli F, Brivio F, Lissoni P, Fumagalli L, et al. (2017) A Study On The Influence Of Spirituality On The Efficacy Of Antitumor Therapies With Natural Anticancer Agents In Untreatable Metastatic Camncer Patients. Cancer Stud Ther J 2: 1-5.
- Lissoni P, Messina G, Rovelli F, Vigorè L, Lissoni A et al. (2018) Low Lymphocyte-To-Monocyte Ratio Is Associated with an Enhanced Regulatory T lymphocyte Function In Metastatic Cancer Patients. Int J Rec Adv Mult Res 5: 3353-3356.
- Paolo Lissoni (2016) Therapy Implications of the Role of Interleukin-2 in Cancer. Expert Rev Clin Immunol 13: 491-498.

