Keywords
ADHD, TCA, methylphenidate, Provocative drugs
Introduction
Attention Deficit Hyperactivity Discarded (ADHD) is a prevalent, continuous and chronic behavioral disorder,
which is seen in 3 to 8 percent of school-aged children and teenagers. And produces problems in patient’s school,
emotional and adaptation performance [11]. However, more completed studies had been conducted in the society
that assessed its real rate between 4 to 12 percent. These studies also indicate that ADHD’s risk in boys compared to
girls is 3 to 1. In average, one child in America in each class room needs help about ADHD [12,13]. This disease
has three man symptoms: excessive activities and motions, desire to make sudden decisions regardless of their result
and lack of attention [14]. Level of these symptoms in children with ADHD varies from a child to the other child.
And all the problems caused by this disorders occurs in all places where the child spent his/ her life like House,
school and social environments and affects child’s life. So no wonder that ADHD causes negative effects on child’s
social behavior, schoolwork and career success.
Children with ADHD have lacking in the ability to sit in class and give sufficient attention to the lessons, so they bring along long and wide negative results. These children are extremely vulnerable [8].
Over the past 10 years, the prevalence of ADHD has been increased significantly. Over time, symptoms
of hyperactivity and inactivity are removed in children, but the lack of attention remains [1].
Research has shown that ADHD tends to spread among families and thus provides evidence that ADHD is a genetic
disease so in the near relatives of the children with ADHD, at least there was one person who already had this
disease. In addition, from the fathers who were diagnosed with ADHD in the young ages, at least one or more of
their children had ADHD. The fact that reveals the role of genetics in causing this disease is that the risk of catching
ADHD in the children who are not twins from their parents is 30 percent but twins have higher risk in comparison
with non-twins. No one exactly knows whether or not, the prevalence of ADHD is increasing? [6,7]
Some forms of behavioral therapy on patients with ADHD, were not beneficial or had very low effects.
These treatments include individual treatment and were based on the child's game, long-term therapy,
development of senses education, and behavioral therapy based on Specific cognitive [9].
But only one of these non-drug perspectives, treatment based on the child’s behavior, in many of children with
ADHD, had significantly beneficial effects [15].
The pharmacological treatment is based on CNS Stimulants prescription. However, in some cases respond to
treatment with these medicines are not suitable or there is even failure in treatment. Alternative medicines for
the treatment of these cases have been considered which includes tricycle antidepressants medicines (TCAs), α2 agonists (Clonidine, Guanfacine) and Norepinephrine reuptake inhibitors (Atomoxotine) and
Amines reuptake inhibitors [10].
Currently the most common treatment is pharmacotherapy. Methylphenidate is usually used in pharmacotherapy but
most of the doctors believe that they are forced to prescribe this medicine because this medicine
only eliminates the symptoms of the disease but it does not cure it and upon discontinuing the medication, symptoms
of the disease appear.
It also has extensive effects on the children’s growth and development of growing [16].
This medicine can also cause cognitive and behavioral disorders [18].
Taking the stimulant medications for ADHD can cause hypertension and tachycardia [19,20]. Considering the
stimulant medicine’s frequent side effects and lack of complete cure for ADHD, we decided to investigate about the
effects of TCA on children with ADHD.
Materials and Methods
A) Disorder diagnosis
ADHD diagnosis is essentially based on the existence of some behaviors like: [21]
1- Inattentiveness: That presents as a lack of concentration, lack of completion of assigned tasks (education), lack
of attention to statements, making frequent mistakes due to carelessness and distraction.
The child is easily distracted and noises or visual stimulus in the environment, will quickly lead to child’s
distraction.
2- Hyperactivity: That presents as constant agitation, wagging the body, moving the legs while sitting and always
having motion. This is an obvious sign of disorder, but may not be available in all cases.
3- Impulsiveness: That presents as uncontrolled and inappropriate responses or inappropriate reactions to occurred
situations and without thinking and risky actions.
4- Typically boys are four times more affected than girls are.
5- Girls mostly have attention deficit without excessive activity.
6-Current classification for the disease is as follow:
A. Mainly the impulsiveness along with hyperactivity
B. Mainly inattentiveness
C. Mixed forms
7-Usually, learning disabilities, aggressive or confrontational behavior are along with this disorder.
Statistical population was selected from referred patients to the children hospital in Tabriz city-East Azerbaijan-
Iran who was suspected of having ADHD between 2010 and 2011.
First patient’s history was prepared and physical examination was taken and results along with patient’s identity,
residence, parental occupation, residence status and economic status information was recorded. While preparing
patient’s history, parental cooperation attracting, ethical standards Observance and explaining about the disorder,
research and how to visit was discussed.
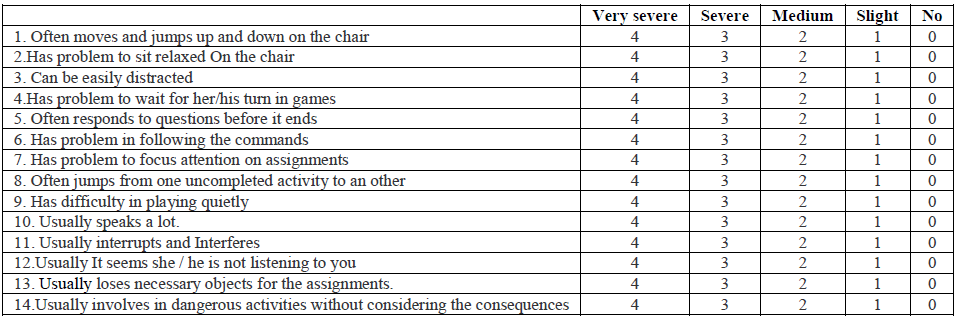
Also for diagnosing disorder, a questionnaire that was answered by the parents has been used. This questionnaire is
based on DSM3R standards and called ADHD Rating Scale [1].
In this questionnaire:
Questions 3, 6, 7, 8, 12 and 13 are the symptoms of inattentiveness.
Questions 1, 2, 3, 6, 7, 8, 12, 13 and 14 are the symptoms of inattentiveness and Hyperactivity.
Questions 1, 2, 4, 5, 9, 10, 11 and 14 are the symptoms of impulsiveness and Hyperactivity.
After selecting patients, people were divided into 2 groups, on each group there were 200 patients. Treatment in the
first group started with short-acting methylphenidate prescription and in the second group started with a TCA
medicine (Imipramine).
Patients every 15 days had a visit and were reviewed, parents answered the same questionnaire, and it was compared
with the previous visit’s questionnaire to assess child’s behavior. Then patients, who had treatment failure after
receiving maximum dose of medicine or demonstrated significant side effects, were changed to the other group. In
cases that failed again in the other group, patients simultaneously received both of the medicines with
moderate doses.
Information about groups:
a. First group included 200 children, 5.5 to 7.5 years old that 170 people were boys (85%) and 30 people were girls
(15%).From 170 boys, 60 patients (35.3%) mainly had Hyperactivity and impulsiveness and inattentiveness and 110
patients (64.7%) were suffering with mixed form of disorder. All 30 girls mainly were suffering from inattention and lack of concentration. To all of them 0.3mg/kg/dose methylphenidate in two sessions was prescribed. In cases where
respond to the treatment was inexpressive to achieve desired results, amount of medicine increased to
0.8mg/kg/dose.
b. The second group included 200 children; 6 to 8 years old that 190 people were boys (95%) and 10 people were
girls (5%). In this group, all people were suffering with mixed form of disorder. For these patients in the first day
imipramine with a dose of 3mg/kg was prescribed and if required it was increased to amount of 5mg/kg per day. At
each visit, from all patients’ blood pressure, CBC dif (from bone marrow suppression) and ECG was measured.
c. During the research, 20 people from first group, 10 girls and 10 boys didn’t cooperate and were excluded from the
study.
d. During the research, 40 boys from first group did not respond to the treatment with the maximum dose of
methylphenidate then they were re-examined, interviewed and assessed in the term of confusion in the diagnosis.
After we ensure about the diagnosis’s accuracy, we replaced them in the third group and changed their treatment to
the TCA medicines.
In the second group, 70 children did not respond to the treatment, and then they were reassessed and after ensuring
about the accuracy of diagnosis, transferred to the third group and treated with methylphenidate.
In all 110 patients in this group, by changing the medicine, results were not acceptable, and for all of them after
reassessing, we started the treatment with moderate doses of both medicines.
Results
• Altogether 400 patients were studied in the research, during the research 20 patients (10 girls and 10 boys) who
were in the first group ,due to not cooperating ,were excluded from the study and further research was
conducted with 380 patients.
From 380 patients, 359 people (92.1%) were boys and 30 people (7.9%) were girls.
Figure 1: sexual breakdown of patients
• In the first group, 160 boys (88.9%) and 20 girls (11.1%), all were treated with short-acting methylphenidate. 41
boys (22.2%) despite increasing the dose of medicine, did not respond to the treatment. But 77.8 % of patients (119
people) responded significantly to the drug in mentioned dose. (P<0.01)
• In the second group, there were 200 children, 190 boys (95%) and 10 girls (5%). In this group, which was
treated with imipramine, 69 people (35%) did not respond to the treatment. Whereas 65% of patients (131 boys)
responded significantly to the drug in mentioned dose (P<0.05).
40 boys from the first group were transferred to the third group and their prescribed medicine was replaced with
methylphenidate instead of imipramine. Only 10 patients (25%) demonstrated good response to treatment.
70 people from the second group, who didn’t respond to the treatment, were transferred to the third group. Their
medicine changed and instead of imipramine, methylphenidate was prescribed for them .30 people (42.8%)
demonstrated good response to the treatment.
Figure 2: frequency of response to treatment with methylphenidate
Figure 3: frequency of response to treatment with imipramine
• In the next step, in the third group, 30 people from first group who had not good response to any of two
medicines along with 40 people from second group who did not respond well to the treatment Had been treated
with moderate doses of both medicine. From 70 patients 50 person (71.4%) demonstrated good respond to the
medicines.
The remaining 20 patients, due to their aggressive behavior that they had from first step, needed other medicines
besides above medicines to control their behavior.
According to the results, it seems that treatment fail is less, in prescribing stimulant medicines (22.2%) compared
with imipramine (35%).
Medication’s replacement from methylphenidate to TCA medicines has no significant impact on increasing respond
to the treatment.
But according to 70 patients (71.4%), who had appropriate respond to two medicines, it seems that in the cases who
do not respond to the treatment with methylphenidate, instead of stopping or changing the medicine, TCA as second
medicine, should be added in the child’s treatment program.
Figure 4: frequency of response to treatment with methylphenidate plus imipramine (P<0.05).
Discussion
Hyperactivity- lack of attention disorder is a common disease, which is seen in children and school-aged teenagers.
In addition, according to the problems, which it created in student’s academic performance, researches about its
therapeutic strategies are so essential.
Satel et al in 1988 conducted a research in a classification, which patients at the same time were suffering with
borderline personality disorder and ADHD. One case was about a young man who had BPD and ADHD and did not
respond to the treatment with methylphenidate, his diseases symptoms such as anxiety, irritability and mood
instability were treated with imipramine. It is proved that Tricycle medicines are helpful for the people who at the
same time are suffering with borderline personality disorder and ADHD [2].
Hilton et al in 1991 conducted a research according to the fact, that fragile X syndrome is the third leading cause to
mental retardation. Thus, a 6-year-old boy with fragile x syndrome, which includes cognitive and
behavioral characteristics of ADHD, and he had insomnia and nocturnal enuresis. These problems previously were
not been reported in fragile X syndrome and the treatment for lack of attention and syndrome behavioral problems,
included stimulation, Folic acid and Neuroleptic. This is the first reported successful use of imipramine.
Imipramine also improved boy’s insomnia and nocturnal enuresis [3].
Ganizadeh et al during the research, which they conducted in 2008, were 40% agreed that ADHD causes
biological and genetic damages. In total, 63% reported irregularities (disorders) are due to poor family performance.
91% believed that ADHD children’s bad behavior is primary, because they do not accept to follow low. According
to the report, 85.5% of used Ritalin increased the focus. 80% of them recommended that Ritalin is the
best treatment. However, 70% reported that, patients despite having Ritalin, had lack of attention and it is not
recommended in ADHD except in exceptional cases [4].
Winsberg BG et al During the research conducted in 1978, prescribed imipramine to 10 children who did not
respond to methylphenidate, but there was no significant medical effect which reduces parents and teachers blame
about child’s behavior and homework.
Obtained results suggest that imipramine limits ADHD’s clinical useful treatment in children who did not respond to
methylphenidate [5].
According to the researches, it seems that, in treating hyperactivity- lack of attention disorder, in patients who are
treating with stimulant medicines and they do not respond to the prescribed medicine, increasing dose of medicine
does not have effect in treatment process. Also in patients who were treated with TCA and do not respond to
prescribed medication, increasing dose of medicine has no effect on treatment process.
In patients, who do not have a proper respond to any of stimulant medicines and TCA, prescribing moderate dose of
both medicine causes improvement in the disease.
According to the result, for responding to the treatment with stimulant medicines, instead of switching or
discontinuing the medicine, second medicine, TCA, should be added to child’s therapy program.
References
- Barkley RA, DuPaul GJ & McMurray MB, Journal of Consulting and Clinical Psychology, 1990, 58, 775-789.
- Satel S, Southwick S, Denton C, J Nerv Ment Dis, 1988, 176, 305-7.
- Hilton DK, Martin CA, Heffron WM, Hall BD, Johnson GL, J Am Acad Child Adolesc Psychiatry, 1991, 30, 831-4.
- Gabriela ML, John DG, Magdalena BV, Ariadna GS, Francisco de LP, Liz SM, Lino PC, Josefina RG, Ernesto RZ, Carlos CF, Neurosci Lett, 2009, 451, 257-60.
- Winsberg BG, Bialer I, Kupietz S, Tobias J, Am J Psychiatry, 1972, 128, 1425-31.
- Asherson P, Gurling H, Curr Top Behav Neurosci, 2011, Oct 12. [Epub ahead of print].
- Larsson H, Anckarsater H, Råstam M, Chang Z, Lichtenstein P, J Child Psychol Psychiatry, 2012, 53, 73-80.
- McLoughlin G, Rijsdijk F, Asherson P, Kuntsi J, Behav Genet, 2011, 41, 668-79.
- Pritchard AE, Nigro CA, Jacobson LA, Mahone EM, [Epub ahead of print], Rev, 2011, Nov 15.
- HP Rang, Dale MM, Ritter JM and Moore PK, Pharmacology, Churchill Livingstone, 2012, 7th Edition, pp 586.
- Greydanus DE, Nazeer A, Patel DR, Neuropsychiatr Dis Treat, 2009, 5, 171-81.
- Nøvik TS, Hervas A, Ralston SJ, Dalsgaard S, Rodrigues Pereira R, Lorenzo MJ, Eur Child Adolesc Psychiatry, 2009, 18, 194-6.
- Ohan JL, Johnston C, Child Psychiatry Hum Dev, 2005, 35, 359-81.
- Erşan EE, Doğan O, Doğan S, Sümer H, Eur Child Adolesc Psychiatry, 2004, 13, 354-61.
- Kakar-Oel A, Forster T, Z Kinder, Jugend psychiatr, 1995, 23, 201-8.
- Moungnoi P, Maipang P, J Med Assoc Thai, 2011, 3, S1, 58-63.
- Lee J, Grizenko N, Bhat V, Sengupta S, Polotskaia A, Joober R, BMC Psychiatry, 2011, 11, 70.
- Wigal SB, Wigal T, Schuck S, Brams M, Williamson D, Armstrong RB, Starr HL, J Child Adolesc Psychopharmacol, 2011, 21, 121-31.
- Samuels JA, Franco K, Wan F, Sorof JM, Pediatr Nephrol, 2006, 21, 92-5.
- Wilens TE, Hammerness PG, Biederman J, Kwon A, Spencer TJ, Clark S, Scott M, Podolski A, Ditterline JW, Morris MC, Moore H, J Clin Psychiatry, 2005, 66, 253-9.
- Sibley MH, Pelham WE, Molina BS, Gnagy EM, Waschbusch DA, Garefino AC, Kuriyan AB, Babinski DE, Karch KM, J Consult Clin Psychol, 2011, 12. [Epub ahead of print].





