Keywords
Clinical manifestations; Chronic LF; Acute necrosis; Jaundice; Liver transplantation
Introduction
Liver failure (LF) is a clinical syndrome characterized by jaundice, coagulopathy, ascites, and hepatic encephalopathy. It is a devastating illness, with extremely high morbidity and mortality rates. Traditionally, LF is classified clinically as acute liver failure (ALF) or chronic liver failure (CLF). More recently, the entity of acute-on-chronic liver failure (ACLF) has been delineated. Pathological changes leading to LF consist of two types: 1) severe acute necrosis of liver tissues and 2) chronic progressive damage to liver cells [1]. The major causes of ALF and CLF are different, which can lead to different clinical manifestations and classification of LF in eastern and western countries: alcohol and drug abuse are the major causes of LF in the West, whereas viral infections are the predominant cause in the East [2].
In recent years, international organizations or societies have issued several guidelines or consensuses about the diagnosis and classification of LF [3-5]. In China, Guidelines for Liver Failure Diagnosis and Treatment were released in 2006 and updated in 2012 by the Liver Failure and Artificial Liver Group of the Chinese association of Infectious Diseases, and the Severe Liver Disease and Artificial Liver Group of the Chinese association of Hepatology [6,7]. These guidelines and consensuses have had a positive effect on LF-related research and academic exchanges worldwide. However, the clinical diagnosis and classification of LF still varies considerably among nations [8,9] and need further clarification.
The Connotation and Pathology of Liver Failure
The connotation of liver failure
Failure of the liver, the center of the body’s metabolism, is not limited to the liver itself, but also has a wide effect on the brain, kidneys, lungs, and other organs. Thus, LF may be considered multi-organ failure. First, we must recognize that LF is a functional diagnosis rather than a disease diagnosis. Second, we should focus on the difference between liver dysfunction and LF. Because the liver has a large reserve capacity and the ability to regenerate, mild or moderate liver damage usually does not result in overt dysfunction.
However, if the damage is more severe and widespread, as for example, from repeated or long-term injury, the resulting metabolic derangements can significantly affect hepatic function. These effects may consist of decreased detoxification of toxic substances, disorders of the formation and excretion of bile, and bleeding tendencies; these in turn may be manifested as jaundice, bleeding, or ascites, and other symptoms or signs. LF is a late stage of liver dysfunction, which may be expressed as hepatic encephalopathy, hepatorenal syndrome, and other disorders [10].
The pathology and clinical significance of liver failure
Studies suggest that pathological changes resulting in LF are of two main types: 1) Acute, severe liver necrosis and 2) chronic, progressive liver-cell damage [1]. There are some differences in pathological changes of LF, especially of ACLF. Some scholars have reported that the pathological changes associated with ACLF may be diverse and dominated by massive or sub-massive necrosis; cirrhosis accompanied with hepatitis may be one expression [11,12]. Li et al. [13] found that sub-massive hepatic necrosis is a pathological feature of hepatitis B virus (HBV)-associated ACLF.
Zhang et al. [14] found that pathological changes associated with ACLF are closely related to duration of disease. In decompensated cirrhosis, 70% of the liver cell function has been lost and is considered CLF [15]; it does not appear as areas or subareas of tissue necrosis. From a prognostic point of view, the significance of the distinction between ACLF and CLF lies mainly with patients who have a component of acute LF that could likely be reversed through liver regeneration. CLF usually is irreversible and may require liver transplantation for effective treatment [16].
Contradiction of Diagnosis and Classification of Liver Failure
Inconsistent LF classification
Although LF has been divided into acute and chronic LF, its classification is dissimilar in various countries and regions of the world. Guidelines and consensus for types of LF come mainly from Europe and the United States: they include the criteria for ALF recommended by the American association for Study of Liver Diseases (AASLD), in 2005 [2]; ACLF consensus released by the Asia-Pacific Association for the study of Liver (APASL), in 2009 [16]; and the consensus on ACLF by AASLD and the European association for the Study of Liver (EASL), in 2011 [4].
The CLF guidelines are non-uniform, only appropriate guidelines or consensus for the complications of cirrhosis, such as ascites, hepatic encephalopathy, and hepatorenal syndrome, have been published [17-19].
Chronic Liver Failure, Mechanisms and Management, edited by Gines et al., were published in 2011 [2]. Williams [20] proposed that LF be divided into three categories: ALF, ACLF, and CLF. According to the Liver Failure Guidelines in China, issued in 2006 and revised in 2012, LF is divided into four categories: ALF, sub-acute LF (SALF), ACLF and CLF (Table 1).
| Three categories (United Kingdom) [20]: ALF, ACLF and CLF |
Four categories (China) [7]: ALF, SALF, ACLF and CLF |
| Definitions |
ALF defined as HE within 8 weeks |
ALF defined as more than Grade II HE within 2 weeks. |
| - |
SALF defined as clinical manifestations of liver failure within a period of 15 days-25 weeks. |
| ACLF defined as acute deterioration of preexisting chronic liver disease, usually related to sepsis, alcohol, or bleeding. |
ACLF defined as acute deterioration on a base of chronic liver disease. (TBil3 171 µmol/L and PTA£40%) |
| CLF defined as progression of end-stage liver disease. |
CLF defined as chronic deterioration of preexisting liver cirrhosis. |
ALF: Acute Liver Failure; SALF: Sub-acute Liver Failure; ACLF: Acute-On-Chronic Liver Failure; CLF: Chronic Liver Failure; HE: Hepatic Encephalopathy; TBIL: Total Bilirubin; PTA:Prothrombin Activity.
Table 1: The current main categories of liver failure and definitions.
The establishment of CLF as a distinct entity is necessary in order to maintain the continuity and integrity of LF classification. However, there is lack of uniformity of CLF guidelines. The cause of this lack might be thought of as the decompensated stage of liver cirrhosis, and appropriate guidelines or consensus for complications of cirrhosis are those mentioned above.
Diagnostic Criteria Differences for Various Types of LF
Given the lack of generally accepted, evidence-based diagnostic criteria, the diagnosis of LF varies within China and between China and other countries. These differences might be due to the variety of causes of LF, the complexity of its clinical manifestations, and differences in expert opinions from various centers. For example, alcoholic cirrhosis constitutes 50% to 70% of all underlying liver diseases of ACLF in western countries, whereas hepatitis B- or C-related cirrhosis constitutes about 10% to 30%. In most Asian countries, however, hepatitis B constitutes about 70% of ACLF, and alcohol abuse only approximatively 15% [21]. These factors notwithstanding, the more important barrier to achieving consensus in LF classification lies in the variations in LF diagnostic standards. For example, the current definition of ACLF differs greatly in various countries. The APASL definition stresses the occurrence of ascites and/or encephalopathy occurring within a period of four weeks in patients with underlying chronic liver disease, whereas the AASLD/EASL definition underlines the occurrence of multi-organ failure in patients with chronic liver disease, resulting in three-month mortality (Table 2). This difference has led to a misconception between ACLF and acute decompensation of liver cirrhosis [22,23]. Moreau et al. [24] reported that ACLF is a different syndrome from that of acute decompensation of cirrhosis. Since the majority of ACLF patients in the Moreau study had alcohol-induced cirrhosis, this conclusion cannot be extended to virus-related ACLF [25]. Because the diagnostic criteria differ significantly, the prognoses of ACLF patients may differ. Thus, Zhang et al. [26] reported that the 90-day mortality rates in the ACLF diagnostic criteria established by APASL, CMA and EASL are 13.1%, 25.3% and 59.3%, respectively. Wang et al. [27] also indicated that the diagnostic criteria for ACLF established by EASL are stringent and may impede early therapeutic intervention. In regard to ALF, Wlodzimirow et al. [28] reported that 41 different definitions of ALF were used in 87 studies. The diversity in definitions of ALF hinders the making of comparisons and quantitative analyses among studies. Whereas there is room for improvement in the reporting of ALF definitions in prognostic studies [28], scholars generally agree on the definition of CLF [6,20].
| LF |
Proposed by |
Definitions |
| ALF |
AASLD (2006) |
No previous history of cirrhosis; deterioration of liver function occurred in 26 weeks; coagulopathy (INR = 1.5);
any degree of altered consciousness (encephalopathy). |
| ACLF |
APASL (2009) |
Acute hepatic insult manifested as jaundice and coagulopathy, complicated within 4 weeks by ascites and/or
encephalopathy in a patient with previously diagnosed or undiagnosed chronic liver disease. |
| |
AASLD/EASL (2011) |
Acute deterioration of preexisting chronic liver disease usually related to a precipitating event and associated
with increased mortality at 3 months due to multisystem organ failure. |
| |
EASL-CLIF Consortium (2013) |
Acute liver deterioration, organ failure (defined by the chronic liver failure-sequential organ failure assessment score)
and high 28-day mortality rate (> 15%) on the basis of acute decompensation of liver cirrhosis |
| |
WGO working party (2014) |
ACLF may be divided into 3 categories depending on whether or not there is underlying cirrhosis and hepatic
decompensation: Type A, non-cirrhotic ACLF; Type B, cirrhotic ACLF; Type C, cirrhotic ACLF with previous hepatic decompensation. |
APASL: Asia–Pacific Association for the Study of the Liver; AASLD-EASL:American Association for the Study of Liver Disease-European Association for the Study of the Liver; ACLF: acute-on-chronic liver failure; CLIF-SOFA: Chronic Liver Failure-Sequential Organ Failure Assessment; INR:International Normalized Ratio; WGO: World Gastroenterology Organization.
Table 2: Definitions of ALF and ACLF by major societies.
Different Pathology Bases of Various Types of LF
Significant differences in understanding of ACLF still exist locally and internationally. Most scholars in Europe and the United States believe that the basic underlying disease is compensated cirrhosis [4,29]. Moreau et al. [24] have stated that decompensated cirrhosis is the basis of ACLF. In China, the ACLF diagnostic criteria take into account the degree of chronic liver disease (e.g., chronic hepatitis and liver cirrhosis), which causes much confusion. ACLF patients have high shortterm mortality. However, those who survive the acute exacerbation live longer than do patients with decompensated cirrhosis [30]. Recently, the World Gastroenterology Organization Working Party suggested that ACLF be divided into 3 categories depending on whether there is underlying cirrhosis and hepatic decompensation: Type A, non-cirrhotic ACLF; Type B, cirrhotic ACLF; Type C, cirrhotic ACLF with previous hepatic decompensation [31]. According to the diagnostic criteria of ALF or subacute LF in China, these types should know the basis of chronic liver disease and are different from ALF as defined by the AASLD [2]. ALF patients have no previous history of cirrhosis, and the deterioration of the liver function occurred within 26 weeks according to the AASLD definition. Also, ALF is characterized by coagulopathy (prothrombin international normalized ratio ≥ 1.5) and any degree of altered consciousness (encephalopathy). For Wilson’s disease, vertical transmission of hepatitis B, or autoimmune hepatitis, disease found at 26 weeks may also be considered ALF even in the presence of cirrhosis. Considering that most Chinese chronic hepatitis B patients are long-term carriers of hepatitis B virus, the first severe occurrence of CHB were regarded as ACLF [32]. Therefore, the current ACLF diagnostic criteria in China might include some ALF due to acute or subacute hepatic necrosis.
Proposed New Classification and Diagnosis of Liver Failure
Given the disagreements of LF diagnosis and classification, the author believes that the diagnosis of hepatic failure must be separated from the clinical classification of complications caused by LF, such as hepatorenal syndrome and hepatic encephalopathy. Although the complications caused by LF are different and have inconsistent manifestations at different stages, the final clinical manifestations are essentially the same. The different stages of the disease are the most significant factors for the prognosis of the patient. Therefore, relaxation of the diagnostic criteria for LF should emphasize prevention in favor of improving patients’ prognosis [33]. For assessing efficacy of treatment, standards should be uniform internationally. Thus, we propose that, based on ALF and CLF, the former be further divided into fulminant-type and subacute-type hepatic failure, and the latter be divided into acute exacerbative type and slowly progressive type (Figure 1) [34]. These criteria of LF are different from the current criteria of the EASL, AASLD and APASL, which might be simpler and more practical.
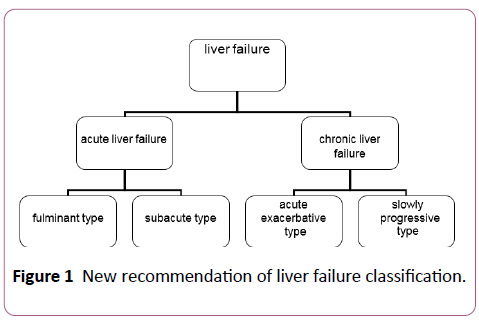
Figure 1: New recommendation of liver failure classification.
ALF
In ALF patients who have more than grade II hepatic encephalopathy, the liver failure progresses rapidly and the prognosis is poor whether or not there is underlying liver disease [35]. This situation is similar to the classic definition of fulminant LF (the mortality rate more than 80%) proposed by Trey [36]. In Asia, including China, some patients have severe jaundice, ascites, and bleeding tendencies, but no hepatic encephalopathy; although their disease progresses relatively slowly, their prognosis is poor (the mortality rate more than 40%~50%). We believe that this condition should be designated subacute LF [37]. Accordingly, ALF could be divided into fulminant and sub-acute types, with the latter having a four-week duration of disease. The designation of fulminant type requires hepatic encephalopathy, whereas the sub-acute type does not necessarily have hepatic encephalopathy and is mainly characterized by severe jaundice and ascites etc.
CLF
Patients with decompensated cirrhosis, because of complications or other factors, may experience either acute deterioration of liver function or slowly progressive disease. Acute deterioration of liver function is defined as the TBil ≥ 171 umol/L and PTA ≥ 40%. Accordingly, CLF can be divided into two types: slowly progressive and acute exacerbative type. The slowly progressive type is equivalent to the current slow progression of decompensated liver cirrhosis in patients with hepatic encephalopathy. Acute exacerbative type is equivalent to deterioration that occurs in decompensated cirrhosis. The short-term prognosis of this type was worse than that of the slowly progressive type [35,38]. Acute exacerbative type might include the ACLF proposed by EASL, which is more serious yet [26].
Conclusion
In summary, considering the numerous causes of LF and clinical manifestations caused by liver damage, differences in the classification of LF are to be expected. Some definitions of LF as ACLF might be conducive to evaluation of short-term prognosis and be harmful to early intervention of disease, versus other definitions. This classification of LF proposed by the author might be more suitable for determining therapy and estimating prognosis. The connotation of ALF and CLF in this classification are different from that of the EASL, AASLD, APASL and China although the name of ALF and CLF are as same as the previous reports [3-7]. Hence, our classifications are new and more rational classification scheme. This classification, if adopted worldwide, could help achieve uniformity in the classification and therapeutic guidelines for liver failure. However, the validity of this classification should be further tested in clinical practice.
References
- Wang YM (2010) New concept in nomenclature, classification and diagnosis of liver failure. Chin J of Hepatol18:803-805.
- Sarin SK, Kumar A, Almeida JA,Bihari C, Chan AC, et al. (2009) Acute-on-chronic liver failure: consensus recommendations of the Asian Pacific Association for the study of the liver (APASL). HepatolInt 3:269-282.
- Polson J, Lee WM (2005) AASLD position paper: The management of acute liver failure. Hepatology 41: 1179-1197.
- Jalan R, Gines P, Olson JC,Mookerjee RP, Moreau R, et al. (2012) Acute-on chronic liver failure. J Hepatol 57: 1336-1348.
- Olson JC, Kamath PS (2011) Acute-on-chronic liver failure: concept, natural history, and prognosis. CurrOpinCrit Care 17: 165-169.
- Liver Failure and Artificial Liver Group (2006) Chinese Association of Infectious Diseases and Severe Liver Disease and Artificial Liver Group, Chinese Association of Hepatology, CMA. Diagnostic and treatment guidelines for liver failure. (2006 Version) Chin J Hepatol 9643-9646.
- Liver Failure and Artificial Liver Group (2012) Chinese Association of Infectious Diseases and Severe Liver Disease and Artificial Liver Group, Chinese Association of Hepatology, CMA. Diagnostic and treatment guidelines for liver failure (2012 version). Chin J of Clin Infect Dis 5:321-328.
- Bowen DG, Shackel NA, Mcccughan GW (2000) East meets West: Acute liver failure in the global village. J of Gastro and Hepatol 15:467-469.
- Graziadei IW (2011) The clinical challenges of acute on chronic liver failure. Liver International31:24-26.
- Wang JZ, YinLH(2007) Pathophysiology.(7th edn).People's Medical Publishing House.Beijing.2: 232-233.
- Hanau C , Munoz SJ, Rubin R (1995)Histopathological heterogeneity in fulminant hepatic failure. Hepatology21:345-351.
- Chong YT, Lin GL, Zhao ZX (2006) Pathological changes of the livers from 39 patients with hepatic failure. Chin J Infect Dis 24 : 172-174.
- Li H, Xia Q, Zeng B, Li ST, Liu H,et al. (2015) Sub-massive hepatic necrosis distinguishes HBV-associated acute on chronic liver failure from cirrhotic patients with acute decompensation. J Hepatol63:50-59.
- Zhang LJ, Wang TL, Liu XH, Zu KJ, Meng X,et al. (2007) Histopathological changes in livers of patients with chronic severe hepatiti B. Chin J Hepatol15: 323-327.
- Gines P, Arroyo V, Kamath PS (2011) Chronic liver failure, mechanisms and management. Humana Press,VII.
- Laleman W, Verbeke L, Meersseman P, Wauters J, Van Pelt J, et al. (2011) Acute-on-chronic liver failure: current concepts on definition, pathogenesis, clinical manifestations and potential therapeutic interventions. Expert Rev GastroenterolHepatol5:523-537.
- https://www.aasld.org/sites/default/files/guideline_documents/adultascitesenhanced.pdf
- European Association for the Study of the Liver (2010) EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J Hepatol 53:397- 417.
- American College of Gastroenterology (2001) Hepatic encephalopathy. Am J Gastroenterol 96:1968-1976.
- Williams R (2007) Acute liver failure-Practical management. ActaGastroenterolBelg70:210-213.
- Kim TY, Kim DJ (2013) Acute-on-chronic liver failure. ClinMolHepatol 19:349-359.
- Bajaj JS (2013)Defining acute-on-chronic liver failure: Will East and West ever meet?Gastroenterol144:1337-1339.
- Sarin SK, Kedarisetty CK, Abbas Z, Amarapurkar D, Bihari C, et al. (2014) Acute-on-chronic liver failure: Consensus recommendations of the Asian Pacific Association for the study of the liver (APASL)2014. HepatolInt 8: 453-471.
- Moreau R, Jalan R, Gines P, Pavesi M, Angeli P, et al. (2013) Acute-on-chronic liver failure is a distinct syndrome that develops in patients with acute decompensation of cirrhosis. Gastroenterol144:1426-1437.
- Wang FS, ZhangZ (2013) How can acute-on-chronic liver failure be accurately identified? Nature RevGastroenterolandHepatol 10: 390-391.
- Zhang Q, Li Y, Han T, Nie C, Cai J, et al. (2015) Comparison of current diagnostic criteria for acute-on-chronic liver failure. PLoS One10:e0122158.
- Wang X, Sarin SK, Ning Q (2015) Definition of ACLF and inclusion criteria for extra-hepatic organ failure. HepatolInt 9:360-365.
- Wlodzimirow KA, Eslami S, Abu-Hanna A, Nieuwoudt M, Chamuleau RA, et al. (2012) Systematic review: acute liver failure - one disease, more than 40 definitions.Aliment PharmacolTher35:1245-1256.
- Wasmuth HE, Kunz D, Yagmur E, Timmer-Stranghöner A, Vidacek D, et al. (2005) Patients with acute on chronic liver failure display ‘sepsis-like’ immune paralysis. J Hepatol 42: 195-201.
- Katoonizadeh A, Laleman W, Verslype C, Wilmer A, Maleux G, et al. (2010) Early features of acute-on-chronic alcoholic liver failure:A prospective cohort study. Gut 59:1561-1569.
- Jalan R, Yurdaydin C, Bajaj JS,Acharya SK, Arroyo V,et al. (2014) Toward an improved definition of acute-on-chronic liver failure. Gastroenterol147:4-10.
- Shi H, Lin GL, Pang YJ,Tian CY (2013) Clinical characteristics and classification of 220 cases HBV related acute on chronic liver failure. Guangdong Medical J 34: 744-746.
- Bernuau J (2004) Acute liver failure: Avoidance of deleterious cofactors and early specific medical therapy for the liver are better than late intensive care for the brain. J Hepatol 41:152-155.
- Sun YL, Zhao JM, Zhou GD, Wang SS, Li WS, et al. (2003) Cut-off period of sub-classification and pathological features of severe hepatitis based on clinical and pathological analyses. Chinese J of Experimental and ClinVirol17: 270-273.
- Xing T, Rentian C, Hao L(2015) New exploration to the clinical classification of liver failure associated with hepatitis B virus. J GastroenterolHepatol Res 4: 1725- 1729.
- Trey C, Davidson CS (1970) The management of fulminant hepatic failure. Prog Liver Dis 3:282-298.
- Acharya SK, Panda SK, Saxena A, Gupta SD (2000) Acute hepatic failure in India: A perspective from the East. J GastroenterolHepatol 15: 473-479.
- Zeng Z, Han YK, Geng H, Ju-Mei C (2006) Reevaluation of the typing criteria for patients with chronic severe hepatitis. Chinese J of Experimental and ClinVirol20:53-55.

