Dhiraj Kumar1*, Girish Sabnis1, Dheeraj More1, Hetan Shah1, Charan Lanjewar1, Prafulla Kerkar1,
Rohit Shriwastav2 and Pradeep Vaideeshwar3
1Department of Cardiology, Seth GS Medical College and KEM Hospital, Mumbai, India
2Department of Internal Medicine, Seth GS Medical College and KEM Hospital, Mumbai, India
3Department of Pathology, Seth GS Medical College and KEM Hospital, Mumbai, India
- *Corresponding Author:
- Dhiraj Kumar
Department of Cardiology, Seth GS Medical College and KEM Hospital
Mumbai, India
Tel: + 91-9323361116
E-mail: dhiraj1645@gmail.com
Received date: March 15, 2018; Accepted date: March 26, 2018; Published date: April 06, 2018
Citation: Kumar D, Shriwastav R, Sabnis G, More D, Shah H, et al. (2018) Catastrophic Sudden Cardiac Death. Are there Lessons to be Learnt? Eur Exp Biol Vol. 8 No. 2:10.
Copyright: © 2018 Kumar D, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: Sudden cardiac death is a catastrophic event which leads to loss of young and middle-aged population with dire consequences. Sometimes, a careful history, physical examination and most importantly electrocardiogram (ECG) can help in suspecting the common causes in young population like underlying channelopathies and cardiomyopathies which can further be diagnosed using echocardiography, cardiac MRI and in some cases genetic tests.
Case summary: A 33-year-old male presented with sycope and ventricular tachycardia leading to death. This patient was diagnosed to have Arrythmogenic right ventricular dysplasia (ARVD) on post mortem pathological examination with features of fatty infiltration and thinning of right ventricular myocardium. Furthermore, on histologically fatty infiltration with inflammatory infiltrates were visualized.
Discussion: Clinical awareness amongst physicians about cardiomyopathies especially ARVD with its subtle yet suggestive ECG changes is the need of the hour. ARVD is a rare disease and can be diagnosed with certainty by analyzing ECG and adding imaging to it. When diagnosed cases are treated appropriately, at least a few cases of sudden cardiac death can be averted.
Keywords
Sudden cardiac death; Arrythmogenic right
ventricular dysplasia; Fatty infiltration; Case report
Introduction
Sudden cardiac death describes an unexpected natural death
from a cardiac cause within a short time period, generally ≤ 1
hour from the onset of symptoms, in a person without any prior
condition that would appear fatal [1]. Although labelled so it is
not always that it happens without warning signs and symptoms.
We describe a case which exemplifies how such catastrophe if not identified in time, can occur with refractory symptoms. Most
of the times a simple history, clinical examination and a 12 lead
ECG is enough to establish a diagnosis [2]. It is also important to
be clinically aware of cardiomyopathies. If a timely diagnosis is
made, then appropriate management can be instituted, and
catastrophe can be prevented.
Clinical Presentation
A 33-year-old farmer while working in his field had a syncope
and was brought to the Emergency Room (ER). On examination
patient had tachycardia and was in cardiogenic shock with a
blood pressure of 70/56 mm of Hg (Figure 1A). His ECG showed
broad complex tachycardia with superior axis and LBBB morphology (Figure 1B).
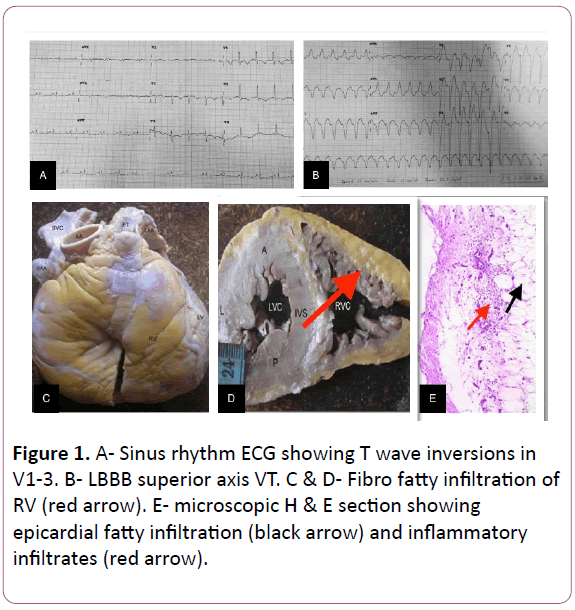
Figure 1: A- Sinus rhythm ECG showing T wave inversions in
V1-3. B- LBBB superior axis VT. C & D- Fibro fatty infiltration of
RV (red arrow). E- microscopic H & E section showing
epicardial fatty infiltration (black arrow) and inflammatory
infiltrates (red arrow).
After 200 Joules of synchronized biphasic direct current (DC)
shock was given, the patient reverted to sinus rhythm. This ECG
showed only T wave inversions in leads V 1-5 (Figure 1A). After
stabilization amiodarone infusion was started. However,
unfortunately the patient had a recurrence of ventricular
tachycardia which degenerated into ventricular fibrillation.
There was no response to DC shock and about 45 minutes of
cardiopulmonary resuscitation and the patient succumbed. An
autopsy was performed.
Histopathology
On gross examination, the right side of the heart showed
yellowish infiltration suggesting fatty or fibro-fatty replacement
starting from epicardium extending into the endocardium with
thinned out myocardium (Figures 1C and 1D). Almost entire muscle layer of right ventricle was replaced by fatty or fibro fatty
tissue. This is the hallmark feature of Arrhythmogenic Right
Ventricular Cardiomyopathy/Dysplasia (ARVC/D). Definite
diagnosis of ARVC requires the histopathologic finding of
transmural fatty or fibro-fatty replacement of RV myocardium
(Figure 1E).
There are two histopathologic variants, namely fatty and
fibro-fatty ARVC/D. In the fatty (or lipomatous) variant, the
adipose tissue reaches the endocardium (transmural infiltration)
and the wall thickness may be normal or even increased
(“pseudo-hypertrophy”). However, a small amount of fibrous
tissue, usually focal, is always present. In the fibro-fatty variant,
the wall is thinner, parchment-like and translucent which
accounts for the saccular aneurysms in the so-called triangle of
dysplasia, a feature that should be considered pathognomonic
of the disease [2].
Discussion
ARVC is an inherited cardiomyopathy characterized by
structural and functional abnormalities of the right ventricular
myocardium with a frequency of approximately 1: 5,000. It is an
autosomal dominant trait with variable penetrance and
incomplete expression. It is an important cause of sudden
cardiac death in young adults accounting for about 11% of all
deaths [3]. Although ARVC requires histopathologic examination
for definitive diagnosis, the typical ECG features and imaging
help to identify patients earlier and prevent sudden cardiac
deaths [4].
The natural history of ARVC/D is highly variable and four
patterns have been proposed [5]:
a) Concealed form, minor arrhythmias, which usually go
unnoticeable. The diagnosis is usually made during family
screening.
b) Overt Electrical Heart disorder, the most typical
presentation, which usually occurs in young patients presenting
with severe and symptomatic ventricular arrhythmias and SCD.
c) RV failure, RV dysfunction with pump failure.
d) Biventricular failure characterized by progressing dilation of
RV and LV; this usually develops late in the natural history of the
c.
A proper ECG screening of patients presenting with
palpitations and syncope will help in identifying many patients
with ARVC/D. There are several ECG features in the criteria
diagnosis of ARVD:
a) T wave inversions in V1 through V3 (minor diagnostic
criterion, but one of most common ECG abnormality present in
85% of patients
b) QRS duration=110 ms in V1 through V3
c) Epsilon wave (electric potentials after the end of the QRS
complex). It is a major diagnostic criterion found in up to 30% of
cases of ARVD.
Other ECG markers of ARVD have been reported: QRS and QT
dispersion, parietal block defined as a QRS duration in leads V1
through V3 that exceeds the QRS duration in lead V6 by >25 ms,
a prolonged S-wave upstroke in V1 through V3=55 ms (it was
seen as the most prevalent ECG feature in 95% of ARVD [6].
Those patients meeting the fixed diagnostic criteria by Marcus
et al. [6] can be used to make a definitive diagnosis and
appropriate management can be instituted [7].
References
- Ackerman M, Atkins D, Triedman J (2016) Sudden Cardiac Death in the Young. Circulation 133: 1106-1026.
- McGregor SM, Aliya N, Husain A (2015) Brief Review and Update of the Clinico-pathologic Diagnosis of Arrhythmogenic Cardiomyopathy. Arch Pathol Lab 139: 1181-1189.
- Corrado D, Link M, Calkins H (2017) Arrhythmogenic Right Ventricular Cardiomyopathy; Review article. N Engl J Med 376: 61-72.
- Thiene G, Nava A, Corrado D (1988) Right ventricular cardiomyopathy and sudden death in young people. N Engl J Med 188: 129-133.
- Corrado D, Basso C, Thiene G, McKenna WJ, Davies MJ, et al. (1997) Spectrum of clinico-pathologic manifestations of arrhythmogenic right ventricular cardiomyopathy/dysplasia: a multicentre study. J Am Coll Cardiol.1997. 30;1512-1520.
- Philips B, Cheng A (2016) Diagnosis and management of arrhythmogenic right ventricular dysplasia. Curr Opin Cardiol 31: 46-56.
- Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, et al. (2010) Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: pro- posed modification of the Task Force Criteria. Eur Heart J 31: 806-814.