Keywords
Oral disinfection; Red LED; Methylene blue; Photodithazine; Photogem; aPDT
Introduction
A healthy oral cavity presents a diverse microbiota, with over 700 species of microorganisms [1]. Such a huge number of microbial species, predominantly bacteria, results in increased risk of nosocomial infections, mostly postoperative pneumonia, when major surgical procedures, such as cardiac surgery, are performed [2]. Oral antiseptics (for example, chlorhexidine) can be used prophylactically, but the reduction of intra-oral bacterial counts is temporary [3]. Prophylactic systemic antibiotics can also be administered prior to procedures, but its use may be associated with unfavourable side effects and increasing bacterial resistance. In this context, new simple and efficient procedures for oral disinfection, such as photodynamic therapy, that could control the oral microbiota without systemic effects should be investigated and its success could add new possibilities for microbial control.
Antimicrobial photodynamic therapy (aPDT) uses a non-toxic drug termed photosensitizer (PS) that is activated by exposure to light of a specific wavelength. In the presence of oxygen, activated PS leads to the production of reactive oxygen species (ROS) that affect the viability of bacterial cells with selective action, targeting only areas with PS accumulation [4,5]. Due to its characteristics, aPDT has no significant side-effects and does not induce bacterial resistance, since bacteria do not develop resistance to ROS [3]. The aPDT have been successfully employed as an adjunctive therapy in periodontitis treatment [6,7], endodontic infections [8] and peri-implant disease [9], and is now under investigation for general oral disinfection [10].
The present clinical study aimed at analyzing aPDT potential in controlling the oral microbiota (mucosa, tongue, saliva), evaluating bacterial recolonization immediately and 30 minutes after the procedure. Our hypothesis was that aPDT could reduce colony-forming units (CFU).
Material and Methods
Experimental groups
Eighty patients presenting gingivitis were selected for this study. The design was approved by the Ethics Committee of the Federal University of Sao Carlos (#058/2011; CAAE 0171.0.135.135-10; process #23112.004838/2010-28, Group III). Inclusion criteria were: to not be under daily use of oral antiseptics; to not be using antibiotics. Patients were randomly divided into 8 groups (10 patients per group), according to the following Table 1.
Table 1 Experimental groups.
| Group |
Treatment |
| G1 |
methylene blue 0.05%+LED |
| G2 |
hydrogen peroxide 3%+methylene blue 0.05%+LED |
| G3 |
Photogem 0.05%+LED |
| G4 |
hydrogen peroxide 3%+Photogem 0.05%+LED |
| G5 |
Photodithazine 0.05%+LED |
| G6 |
Photodithazine 0.05% |
| G7 |
chlorhexidine 0.12%+LED |
| G8 |
chlorhexidine 0.12% (control group) |
Drugs
Photosensitizers: methylene blue 0.05% (Sigma-Aldrich Co. LLC, St. Louis, MO, USA); Photodithazine® 0.05% (Moscow, Russia); Photogem® 0.05% (Moscow, Russia).
Chlorhexidine 0.12% (Periogard®, Colgate, Brazil).
Hydrogen peroxide 3% (Vic Pharma, Taquaritinga, SP, Brazil)
Experimental procedure
1. Saliva sampling: Prior to treatments, samples of saliva were collected from each patient and named “baseline” of microbiological concentration.
2. Mouth rinse: The patients received in a disposable cup containing 10 mL of a mouth rinse solution, according to their experimental group. They were asked to rinse for 30 seconds and then spit the solution.
3. Irradiation: Light irradiation took place 5 minutes after mouth rinse. The light source was a prototype composed of 3 combined tips each containing a light emitting diode (LED) emitting at 640 ± 5 nm, with a total intensity of 180 mW/cm² (Figure 1). The prototype was introduced into the mouth for 15 minutes, resulting in an energy density of 60 J/cm². To avoid patient-to-patient contamination, the tips were covered with plastic films before each irradiation (Figure 2).
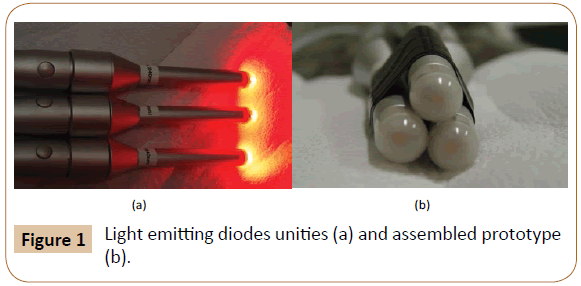
Figure 1: Light emitting diodes unities (a) and assembled prototype (b).
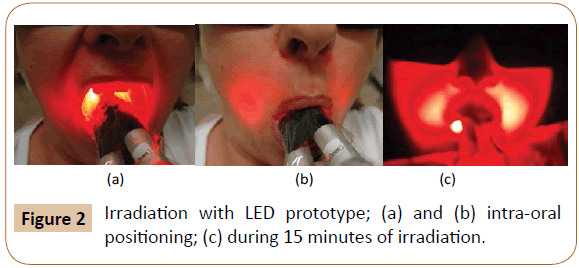
Figure 2: Irradiation with LED prototype; (a) and (b) intra-oral positioning; (c) during 15 minutes of irradiation.
4. Immediately after irradiation, saliva samples were collected and again 30 minutes after the treatment.
Microbial cultivation and decontamination assessment
After collection, samples were temporarily conserved in sterile microtubes and immediately sent to the microbiology laboratory, where they were submitted to 6 serial dilutions (1:10) in saline solution. Following, all 6 dilutions (10-1 - 10-6) were plated into Blood Brain Heart Infusion agar. Plates were incubated at 37°C under microaerophilic conditions for 48 hours. After incubation, colony forming units (CFU) were determined. Post-treatment samples were compared to baseline samples of each patient.
Statistical analysis
Data were expressed as the mean plus standard deviation (SD). To compare the changes between pre- and post-treatment periods data were analyzed by two-way ANOVA with Bonferroni post hoc. To compare changes among groups data were analyzed by oneway ANOVA with Tukey’s post hoc, using the software Statistica for Windows Release 7 (Statsoft Inc., Tulsa, Ok, USA). Differences were considered to be significant when p<0.05 (confidence level of 95%) (Table 2).
Table 2 Log10 of colony forming units obtained for the three different periods.
| Treatment |
Baseline |
Immediately after |
30 minutes after |
| Mean |
SD |
Mean |
SD |
Mean |
SD |
| (G1) (methylene blue+LED) |
8.03 |
0.30 |
7.70 |
0.40 |
7.70 |
0.22 |
| (G2) (H2O2+methylene blue+LED) |
6.97 |
0.60 |
6.33* |
0.58 |
6.77‡ |
0.36 |
| (G3) (Photogem+LED) |
7.55 |
7.36 |
6.27 |
6.30 |
6.42 |
6.40 |
| (G4) (H2O2+Photogem+LED) |
7.11 |
0.26 |
5.29 |
1.44 |
6.67 |
0.45 |
| (G5) (Photodithazine) |
7.34 |
0.41 |
6.75 |
0.22 |
6.79 |
0.07 |
| (G6) (Photodithazine+LED) |
6.71 |
0.42 |
5.37** |
1.85 |
5.14** |
2.24 |
| (G7) (chlorexidine+LED) |
6.59 |
0.26 |
6.00 |
0.08 |
6.56 |
0.02 |
| (G8) (chlorexidine) |
7.42 |
1.39 |
4.13** |
2.18 |
6.45‡‡ |
0.67 |
*Significant difference compared to baseline .
**Significant difference compared to baseline.
‡Significant difference compared to immediately post-treatment .
‡‡Significant difference compared to immediately post-treatment .
Results
As expected, chlorhexidine did not have its activity improved upon light exposure (G7). Chlorhexidine does not absorb light in the wavelength range emitted by the red LED, and, therefore, the irradiation has no effect on its bactericidal activity.
When the mouth rinse procedure was composed of rinsing with hydrogen peroxide prior to the photosensitizer solution (G2 and G4), the bacterial reduction was more significant immediately after the procedure in comparison with their counterpart groups (G1 and G3, respectively), in accordance with Garcez et al. [11]. Those results indicate that the bactericidal effect is boosted when an oxidizing solution is applied before the aPDT.
Compared to the control group (G8), groups G4 and G6 provided the best results, with G6 being the most promising alternative for oral disinfection, since the treatment with Photodithazine was able to sustain the bacterial reduction for at least 30 minutes, a feature not observed for any other group.
Discussion
Oral decontamination can have a direct impact on the outcome of major surgical procedures, the health of critically ill patients intubated for prolonged periods [2], and on situations in which the patient is unable to perform adequate oral hygiene unattended, either by presenting restricted conscious movements or being unconscious.
Current decontamination procedures include oral antiseptics (mostly chlorhexidine) and/or prophylactic systemic antibiotics, but their use may be associated with unfavorable side effects and increasing bacterial resistance, besides producing only a temporary bacterial reduction [3]. In this context, new simple and efficient procedures to promote general oral decontamination, without the need of an effort from the patient, which could control the oral microbiota without systemic effects must be investigated.
In this way, the technique described here is really appealing, considering that it employs a simple photosensitizer mouthwash and subsequent irradiation under an adequate parameter, resulting in a significant microbiological control that lasts for at least 30 minutes after the procedure, an indication of an impairment in oral recolonization.
Although chlorhexidine, the standard mouthwash for oral antiseptics, presented the best result immediately after the procedure, decontamination was not sustained, with recolonization occurring within 30 minutes. In general, aPDT presents a smaller overal decrease, but with clear longer term sustained level of decontamination. In addition, the association of hydrogen peroxide as a mouth rinse prior to PS rinse improved the outcome, reducing bacterial counts in over 1 log10 (>90%). However, aPDT with Photodithazine, without hydrogen peroxide, resulted in a bacterial reduction of 3 log10 (99.9%) after the procedure, proving to be the best treatment for general oral decontamination with longer sustained result.
Besides decontamination, all patients from the groups with aPDT reported improvement in gingivitis and reduction of gum bleeding after treatments. In addition, some patients reported that after the aPDT session they did not observe bleeding upon brushing; teeth presenting hypersensitivity to cold had sensitivity decreased; patients who were with a sore throat and pain had both conditions resolved; one patient reported cure of sinusitis, and another patient who suffered from mentonian paresthesia showed recovery. All improvement reports can be associated both with the reduction of local infection and the benefits of red light itself, including local lymphatic drainage, reducing inflammation and accelerating cell differentiation.
The results presented here provide clear evidence of aPDT as an already possible technique for clinical use with a lot of possibilities for improvements. Variations of incubation time, as well as better illumination devices to better cover the oral cavity geography, would certainly improve the procedure in one to two orders of magnitude, achieving closer results as observed for the traditional procedures, with the advantage of obtaining a longerterm sustained decontamination level.
Conclusion
Antimicrobial photodynamic therapy is a low-cost approach and seems to be reliable for oral decontamination. Within the photosensitizers tested in this study, Photodithazine seems to be the best PS due to the longer sustained bacterial reduction obtained after the treatment. These findings could impact patient preparation prior to major surgery procedures and patient health in intensive care units.
Funding
This research was funded by CNPq - RHAE Process 552720/2009-7.
Acknowledgements
We would like to thank the post-doc fellow Fernanda Paolillo for the statistical analysis and the doctorate student Layla Pires for the microbiology analysis, both from the Biophotonic Lab – IFSC/ USP.
Compliance with ethical standards
This study design was approved by the Ethics Committee of the Federal University of São Carlos (#058/2011; CAAE 0171.0.135.135- 10; process #23112.004838/2010-28, Group III) and was conducted in accordance with the Declaration of Helsinki. All patients read and signed an informed consent prior to joining the study.
Conflicts of Interest
Authors declared that there are no conflicts of interest.
References
- Avila M, Ojcius DM, Yilmaz O (2009) The oral microbiota: living with a permanent guest. DNA Cell Biol 28: 405-411.
- Spreadborough P, Lort S, Pasquali S, Popplewell M, Owen A, et al. (2016) A systematic review and meta-analysis of perioperative oral decontamination in patients undergoing major elective surgery. Perioperative Medicine 5: 6.
- Takasaki AA, Aokia A, Mizutani K, Schwarz F, Sculean A, et al. (2009) Application of antimicrobial photodynamic therapy in periodontal and peri-implant diseases. J Periodontal 51: 109-140.
- de Oliveira RR, Schwartz-Filho HO, Novaes AB Jr, Taba M Jr (2007) Antimicrobial photodynamic therapy in the non-surgical treatment of aggressive periodontitis: a preliminary randomized controlled clinical study. J Periodontal 78: 965-973.
- de Oliveira RR, Schwartz-Filho HO, Novaes AB, Garlet GP, de Souza RF, et al. (2009) An antimicrobial photodynamic therapy in the non-surgical treatment of aggressive periodontitis: cytokine profile in gingival crevicular fluid, preliminary results. J Periodontal 80: 98-105.
- Andrade CPV, Alves EVT, de Carvalho VF, Rodrigues DFM, Pannuti CM, et al. (2016) Photodynamic therapy decrease immune-inflammatory mediators’ levels during periodontal maintenance.
- de Freitas LM, Calixto GM, Chorilli M, Giusti JS, Bagnato VS, et al. (2016) Polymeric Nanoparticle-Based Photodynamic Therapy for Chronic Periodontitis in Vivo. Int J Mol Sci 17: E769.
- Garcez AS, Arantes-Neto JG, Sellera DP, Fregnani ER (2015) Effects of antimicrobial photodynamic therapy and surgical endodontic treatment on the bacterial load reduction and periapical lesion healing. Three years follow up. Photodiagnosis Photodyn Ther 12: 575-580.
- Vohra F, Al-Rifaiy MQ, Lillywhite G, Abu Hassan MI, Javed F (2014) Efficacy of mechanical debridement with adjunct antimicrobial photodynamic therapy for the management of peri-implant diseases: a systematic review. Photochem Photobiol Sci 13: 1160-1168.
- Leite DP, Paolillo FR, Parmesano TN, Fontana CR, Bagnato VS (2014) Effects of photodynamic therapy with blue light and curcumin as mouth rinse for oral disinfection: A randomized controlled trial. Photomed Laser Surg 32: 627-632.
- Garcez AS, Núñez SC, Baptista MS, Daghastanli NA, Itri R, et al. (2011) Antimicrobial mechanisms behind photodynamic effect in the presence of hydrogen peroxide. Photochem Photobiol Sci 10: 483-490.