Paolo Lissoni*, Vichy Cenaj, Franco Rovelli, Giusy Messina, Giorgio Porro, Fernando Brivio and Giuseppe Di Fede
Institute of Biological Medicine, Milan, Italy
*Corresponding Author:
Paolo Lissoni
Institute of Biological Medicine
Milan, Italy
Tel: +39 02 5830 0445
E-mail: paolo.lissoni@gmx.com
Received Date: 09 September 2017; Accepted Date: 06 October 2017; Published Date: 10 October 2017
Citation: Lissoni P, Cenaj V, Rovelli F, Messina G, Porro G, et al. (2017) A Study on the Endocrine Function of Pineal Gland With Regard To Immune Alterations in Cancer Patients. Res J Oncol. Vol. 1 No. 1: 2.
Copyright: © 2017 Lissoni P, et al. This is an open-access article distributed under the terms of the creative Commons attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Keywords
Cancer; Lymphocyte-to-monocyte ratio; Melatonin; Pineal gland; 6-sulfatoxymelatonin
Introduction
Despite the well demonstrated anticancer role of the pineal gland in experimental conditions [1-3], very few clinical studies have been performed up to now to evaluate the pineal endocrine function in cancer patients [4,5]. In any case, either in animals or in humans, cancer progression has appeared to be constantly associated with a progressive deficiency in the pineal endocrine function, as shown by the progressive decline in the production of the most investigated pineal hormone, the indole hormone melatonin (MLT), which has been proven to play a physiological anticancer activity through either a direct cytotoxic action, or an immunostimulatory effect on the anticancer immunity [6,7]. In more detail, MLT antitumor cytotoxic action is due to several mechanisms, the most important of them are consisting of the induction of tumor cell apoptosis and the inhibition of the action of several tumor growth factors. At the other side, the stimulatory effect of MLT on the anticancer immunity is mainly depending on a stimulation of the main antitumor cytokines in humans, consisting of IL-2 and IL-12. In normal conditions, MLT is mainly secreted during the dark period of the day [8], with a following well defined light/dark circadian rhythm in MLT secretion. MLT, however, is not the only hormone responsible for the anticancer activity of the pineal gland, since at least two other pineal hormones have appeared to exert a direct anticancer cytotoxic action, consisting of the indole 5- methoxytryptamine [9] and the beta-carboline pinoline [10]. Moreover, histological damages of the pineal gland have been demonstrated in patients died from cancer [11]. Therefore, the progressive decline in MLT secretion would not represent the only pineal endocrine deficiency with cancer progression. Therefore, the pineal endocrine deficiency would constitute one of the main biological alterations responsible for cancer onset and development. The pineal endocrine deficiency could either precede or promote cancer development, or be induced by cancer dissemination. Pineal deficiency may predispose to tumor onset, since it has been demonstrated that a pineal deficiency induced by surgical or pharmacological pinealectomy has been proven to promote cancer development, whereas the administration of pharmacological doses of MLT has appeared to reduce the incidence of both spontaneous and chemically-induced tumors [12]. In fact, all psychological conditions predisposing to cancer, including stress, depression, pleasure repression and changes in light/ dark rhythm, are constantly characterized by potential alterations in the pineal endocrine function [8-12]. On the other hand, tumor cells may directly produce the enzyme 2, 3- indole-dioxygenase (IDO) [13], which is able to induce tryptophan depletion and a consequent pineal endocrine deficiency, since all pineal hormones originate from tryptophan itself. In addition to the pineal endocrine deficiency, another fundamental biological alteration stimulating cancer growth is the lack of an effective anticancer immune reaction. Despite its complexity, it is currently known that the anticancer immune response in humans is substantially due to T helper-1 (TH1) lymphocytes through the release of IL-2 and to dendritic cells by the secretion of IL-12 [14,15]. IL-2 plays an anticancer activity by inducing the evolution of NK cells into LAK cells, which are able to destroy fresh human cancer cells irrespectively of their antigenicity [16]; IL-12 instead is able to counter cancer cell proliferation by stimulating cytotoxic T lymphocytes, which exercises an antigen-dependent cytotoxicity, by promoting T lymphocyte differentiation into TH1 cells, by counteracting the generation of regulatory T lymphocytes (T reg) [17], which in contrast suppress the antitumor immunity [18], and by playing an antiangiogenic activity. MLT stimulates the anticancer immunity through several mechanisms, which may be synthetized into three essential effects: stimulation of IL-2 release from TH1 lymphocytes, stimulation of IL-12secretion by dendritic cells [7] and inhibition of T reg cell generation [19]. Therefore, due to the stimulatory effect of MLT on the anticancer immunity, cancer-progression related immunodeficiency could depend at least in part on the pineal endocrine failure. Up to now, however, there are no data available on the possible relationship between cancer-related pineal deficiency and immune alterations, which may characterize the advanced neoplastic diseases. Until a few years ago, the clinical evaluation of the immune status of cancer patients required several and expensive immune detections, including the measurement of lymphocyte subsets and cytokine blood concentrations. Recent studies, however, have demonstrated that the simple lymphocyte-to-monocyte ratio (LMR) may reflect the interaction between the anticancer immune reaction, which is mainly mediated by lymphocytes, and the chronic inflammatory status, which is mediated by the monocyte-macrophage system and which suppresses the anticancer immunity by allowing the generation of T reg lymphocytes. Therefore, abnormally low LMR values represent a sign of immunosuppression of anticancer immunity. For this reason LMR may be a simple and inexpensive biomarker for the clinical follow-up of the of anticancer immunity status in cancer patients in relation to the response to the various antitumor therapies and to the clinical course of the neoplastic disease. The present study was performed to investigate which relation may exist between the pineal endocrine function, evaluated by detecting MLT secretion, and the immune status, as synthetized by evaluating LMR, in a group of cancer patients with locally limited or metastatic disease.
Patients and Methods
The study included 30 consecutive cancer patients affected by the most common neoplasms, 16 of whom showed a metastatic disease. Eligibility criteria were, as follows: histologically proven solid tumor, measurable lesions, and no therapy with drugs potentially influencing MLT secretion from at least 1 week prior to study, including corticosteroids, opioids, beta-blockers and alpha-2 agonists. The clinical characteristics of patients are reported in Table 1. MLT secretion was assessed by measuring the urinary daily excretion of its main metabolite, the 6-sulphatoxy melatonin (6-MTS), by comparing the values observed during the light (8.0 AM-8.0 PM) and the dark (8.0 PM-8.0 AM) period of the day. 6-MTS was detected by a commercially available enzyme immunoassay kits (Melatonin-Sulfate Urine – ELISA, IBL INTERNATIONAL GMBH / Tecan Group Company) and the values were reported as mcg/ml. The circadian rhythm of MLT was considered to be within the normal range when 6-MTS values of the dark urinary sample were at least two times greater than those of the light sample. Finally, LMR values were considered to be normal when they were greater than 2.1 (95% confidence limits). Data were reported as mean ± SE, and statistically analyzed by the chi-square test, and the Student’s t test, as appropriate.
Table 1Clinical characteristics of 30 solid tumor patients.
| Characteristics |
n |
| Sex (M/F) |
13/17 |
| Median age (years) |
62 (37-81) |
| Tumor histotype |
| Breast cancer |
10 |
| Lung cancer |
4 |
| Colorectal cancer |
4 |
| Gastric cancer |
3 |
| Pancreatic cancer |
3 |
| Ovarian cancer |
3 |
| Sarcoma |
3 |
| Disease extension |
| Locally limited disease |
14 |
| Metastatic disease (Dominant sites) |
16 |
| Soft tissues |
3 |
| Bone |
2 |
| Lung |
2 |
| Liver |
3 |
| Peritoneum |
3 |
| Brain |
3 |
Results
A normal 6-MTS rhythm, with night values at least greater two times than the light ones, was present in only 14/30 (47%) patients. Moreover, the percentage of patients with normal pineal rhythm observed in the non-metastatic group was significantly higher with respect to that found in the metastatic group (10/14 (71%) vs. 4/16 (25%), P<0.01). Abnormally low values of LMR were seen in 11/30 (37%) patients, and the percentage of patients with low LMR values was significantly higher in the metastatic group than in the non-metastatic one (3/14 (21%) vs. 8/16 (50%), P<0.01). Moreover, the percentage of patients with normal pineal rhythm was significantly higher in the group of patients with normal LMR values than in those with abnormally low LMR values (11/19 (59%) vs. 3/11 (27%), P<0.05). On the other side, the percentage of normal LMR values observed in the group of patients with normal 6-MTS rhythm was significantly higher than that found in patients, who had no rhythm (12/14 (86%) vs. 7/16 (44%), P<0.01). Furthermore, patients with normal 6- MTS rhythm showed significantly higher mean values of LMR than those found in patients, in whom the rhythm was absent (4.7 ± 0.4 vs. 2.3 ± 0.3, P<0.01). Day and night 6-MTS urinary values observed in non-metastatic and in metastatic patients, as well as in patients with normal or abnormally low LMR values are illustrated in Figure 1. In patients with locally limited tumor, a light/dark rhythm was still present, with night mean values of 6-MTS significantly higher with respect to those found during the light period of the day (P<0.025). Conversely, no circadian rhythm in 6- MTS production was seen in metastatic patients, since there was no significant difference between day and night 6-MTS mean values. Night mean values of 6-MTS observed in non-metastatic patients were significantly higher than those found in metastatic patients (P<0.05). Likewise, night mean values of 6-MTS observed in patients with normal LMR values were significantly higher than those found in patients with low LMR values (P<0.05), while no significant difference occurred in 6- MTS mean values during the light period of the day.
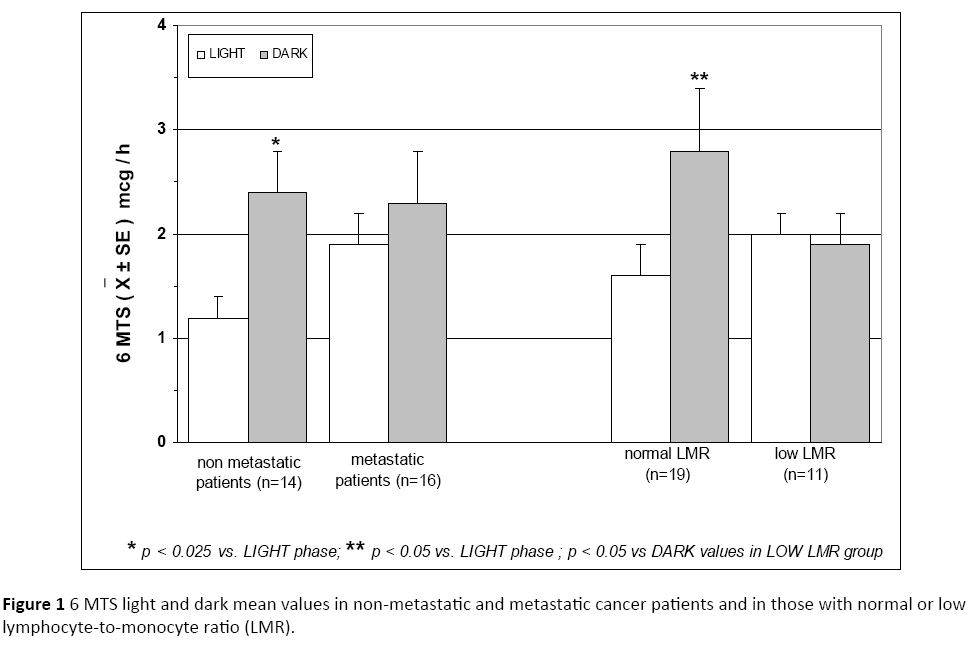
Figure 1: 6 MTS light and dark mean values in non-metastatic and metastatic cancer patients and in those with normal or low lymphocyte-to-monocyte ratio (LMR).
Discussion
As in previous preliminary experimental and clinical investigations, this study confirms that cancer progression is associated with a progressive decline in the nocturnal pineal production of MLT, with a consequent progressive loss of the natural resistance against cancer growth, which is mainly mediated by the pineal gland and the immune system. Moreover, this study also confirms that cancer dissemination is constantly characterized by profound immune alterations, as shown by the evidence of a decline in LMR values in metastatic patients, confirming that cancer progression is associated with a progressive decline in lymphocyte functions and with a concomitant increase in monocyte-macrophage system activation, that mediates the suppression of the anticancer immunity by allowing the generation of T reg cells [20].
Conclusion
Finally, this study shows that there is an association between pineal and immune alterations, because of the evidence of a greater percentage of immune alterations in those patients, who had no light/dark circadian rhythm in the pineal endocrine function. Therefore, cancer progressionrelated alterations in the antitumor immunity would depend, at least in part, on the progressive decline in the pineal endocrine function. This finding is not surprising considering the stimulatory role of MLT on the generation of an effective anticancer immune reaction through the activation of TH1 lymphocyte functions and the inhibition of the monocytemacrophage system [21]. Therefore, cancer therapy with MLT could represent a new antitumor treatment, capable of acting at the same time either as an endocrine therapy, or as an immunotherapy by inducing an effective anticancer immune reaction through a modulation of the same mechanisms responsible for the central psycho-neuro endocrine regulation of the immune system, including the anticancer immunity [22]. Obviously, further clinical studies will be required to in vivo confirm the great number of immune effects induced by MLT, namely by monitoring changes in lymphocyte subsets and in the blood levels of those cytokines mainly involved in the control of the inflammatory response and the antitumor immunity, including the antitumor cytokines IL-2 and IL-12, and the immunosuppressive ones IL-10 and TGF-beta. If further studies will confirm the capacity of MLT to pilot the cytokine network in an antitumor way, MLT could be successfully used in association with the recent anticheckpoint inhibitor immunotherapies of cancer.
Acknowledgments
The authors sincerely thank Dr. Sa Monica Raggi (Lab. of Microbiology, San Gerardo Hospital, Monza, Italy) for her support in the translation of the present work.
References
- Buswell RS (1975) The pineal and neoplasia. Lancet 1: 34-35.
- Regelson W, Pierpaoli W (1987) Melatonin: a rediscovered antitumor hormone? Cancer Invest 5: 379-385.
- Reiter RJ (2004) Mechanisms of cancer inhibition by melatonin. J Pineal Res 37: 213-214.
- Di Bella L, Scalera G, Rossi MT (1979) Perspectives in pineal function. Prog Brain Res 52: 475-477.
- Bartsch C, Bartsch H (1999) Melatoin in cancer patients and in tumor-bearing animals. Adv Exp Med Biol 467: 247-264.
- Maestroni JGM (1993) The immunoneuroendocrine role of melatonin. J Pineal Res 14: 1-10.
- Guerrero JM, Reiter RJ (2002) Melatonin-immune system relationships. Curr Topics Med Chem 2: 167-180.
- Brzezinski A (1997)Melatonin in humans. N Engl J Med 336: 186-195.
- Sze SF, Ng TB, Liu WK (1993) Antiproliferative effect of pineal indoles on cultured tumor cell lines. J Pineal Res 14:27-33.
- Song Y, Wang J, Teng SF, Kesuma D, Deng Y, et al. (2002) Beta-carbolines as specific inhibitors of cyclin-dependent kinases. Bioorg Med Chem Lett 12: 1129-1132.
- Hadjiu SI, Porro RS, Lieberman PH (1972) Degeneration of the pineal gland of patients with cancer. Cancer 29: 706-709.
- Conti A, Maestroni JGM (1995) The clinical immunotherapeutic role of melatonin in Oncology. J Pineal Res 129: 103-110.
- Mittal D, Gubin MM, Schreiber RD, Smyth MJ (2009) Insights into cancer immunoediting and its three component phases-elimination, equilibrium and escape. Curr OpinImmunol 27: 16-25.
- Atzpodien J, Kirchner H (1990) Cancer, cytokines and cytotoxic cells: Interleukin-2 in the immunotherapy of human neoplasms. Klin Wochenschr 68: 1-11.
- Banks RE, Patel PM, Selby PJ (1999) Interleukin-12: A new clinical player in cytokine therapy. Br J Cancer 80: 407-411.
- Grimm EA, Mazumder A, Zhang HZ, Rosenberg SA (1982) Lymphokine-activated killer cell phenomenon. J Exp Med 155: 1823-1841.
- Prochazkiva J, Pokoma K, Holan V (2012) IL-12 inhibits the TGF-beta-dependent T cell developmental programs and skews the TGF-beta-induced differentiation into a Th1-like direction. Immunobiology 217: 74-82.
- Zou W (2006) Regulatory T cells, tumor immunity and immunotherapy. Nat Rev Immunol 6: 295-307.
- Liu H, Wei JE, Xie MR, Wang SE, Zhou RX (2011) Role of CD4+CD25+ regulatory T cells in melatonin-mediated inhibition of murine gastric cancer cell growth in vivo and in vitro. Anat Rec (Hoboken) 294: 781-788.
- Eo WK, Chang HJ, Kwon SH, Koh SB, Kim YO, et al. (2016) The lymphocyte tomonocyte ratio predicts patient survival and aggressiveness of ovarian cancer. J Cancer 7: 289-296.
- Mantovani A, Allavena P, Sica A, Balkwill F (2008) Cancer-related inflammation. Nature 454: 436-444.
- Lissoni P (1999) The pineal gland as a central regulator of cytokine network. Neuroendocrinol Lett 20: 103-110.

